Yang Siran, Xiao Jianping, Liu Qingfeng, Zhang Ye, Bi Nan, Huang Xiaodong, Chen Xuesong, Wang Kai, Ma Yuchao, Deng Lei, Wang Wenqing, Zhao Ruizhi, Li Junling, Yi Junlin, Wang Shulian, Li Yexiong
Department of Radiation Oncology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China.
Department of Medical Oncology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China.
Front Oncol. 2021 Oct 14;11:732883. doi: 10.3389/fonc.2021.732883. eCollection 2021.
The high intracranial efficacy of targeted therapeutic agents poses a challenge in determining the optimal sequence of local radiation therapy (RT) and systemic treatment with tyrosine kinase inhibitors (TKIs) in non-small cell lung cancer (NSCLC) patients with brain metastasis (BM). Therefore, we conducted a cohort study to elucidate the appropriate treatment strategy, either upfront RT or deferred RT including a toxicity assessment, in these patients.
We retrospectively evaluated patients with gene-driven BMs from a single institution and divided them into deferred and upfront RT groups. Survival was estimated using a log-rank test. Intracranial progression was estimated using Fine-Gray competing risks model. Cox proportional hazards regression was performed for multivariable analysis in the entire group and subgroups.
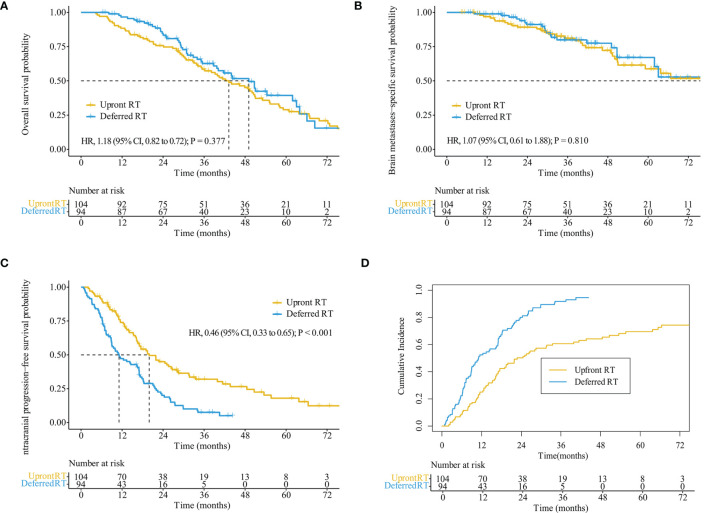
Among the 198 eligible patients, 94 and 104 patients received deferred and upfront RT, respectively. The upfront RT group showed a lower intracranial progression risk with an adjusted sub-distribution hazard ratios of 0.41 (95% CI, 0.30-0.57) than did the deferred RT group (median intracranial progression-free survival [iPFS], 19.9 months 11.1 months; < 0.001). The median overall survival (OS; 43.2 months 49.1 months, = 0.377) and BM-specific survival (92.1 months 82.9 months, = 0.810) after salvage therapy were not significantly different between the upfront and deferred groups. Among patients with progressed extracranial disease, the deferred RT group showed significantly better OS than did the upfront RT group (44.0 28.1 months, = 0.022). Grade 3-4 treatment-related adverse events were rare, and similar toxicities were observed between the two groups.
Compared to the deferred RT group, the upfront RT group achieved longer iPFS and similar survival outcomes in most patients with gene-driven NSCLC BM, although patients with progression of extracranial disease might benefit from deferred RT. Both groups showed well-tolerated toxicities.
NCT04832672.
在非小细胞肺癌(NSCLC)脑转移(BM)患者中,靶向治疗药物的高颅内疗效给确定局部放射治疗(RT)与酪氨酸激酶抑制剂(TKIs)全身治疗的最佳顺序带来了挑战。因此,我们开展了一项队列研究,以阐明这些患者合适的治疗策略,即先行RT还是延迟RT,同时进行毒性评估。
我们对来自单一机构的基因驱动型BM患者进行回顾性评估,并将他们分为延迟RT组和先行RT组。采用对数秩检验估计生存率。使用Fine-Gray竞争风险模型估计颅内进展情况。对整个组和亚组进行Cox比例风险回归以进行多变量分析。
在198例符合条件的患者中,分别有94例和104例患者接受了延迟RT和先行RT。先行RT组的颅内进展风险较低,调整后的亚分布风险比为0.41(95%CI,0.30 - 0.57),低于延迟RT组(颅内无进展生存期[iPFS]中位数,19.9个月对11.1个月;P < 0.001)。先行组和延迟组在挽救治疗后的总生存期(OS;43.2个月对49.1个月,P = 0.377)和BM特异性生存期(92.1个月对82.9个月,P = 0.810)无显著差异。在颅外疾病进展的患者中,延迟RT组的OS显著优于先行RT组(44.0对28.1个月,P = 0.022)。3 - 4级治疗相关不良事件罕见,两组观察到的毒性相似。
与延迟RT组相比,先行RT组在大多数基因驱动型NSCLC BM患者中实现了更长的iPFS和相似的生存结果,尽管颅外疾病进展的患者可能从延迟RT中获益。两组的毒性耐受性均良好。
NCT04832672。