Bayón J C, Orruño E, Portillo M I, Asua J
1Basque Office for Health Technology Assessment (OSTEBA), Ministry of Health, Basque Government, c/Donostia 1, 01010 Vitoria-Gasteiz, Basque Country Spain.
Bioaraba Health Research Institute, Methodology and Statistics Unit, Araba University Hospital, Txagorritxu Headquarters, 4th Floor, c/José Achótegui, 01009 Vitoria-Gasteiz, Basque Country Spain.
Cost Eff Resour Alloc. 2019 Mar 1;17:6. doi: 10.1186/s12962-019-0173-8. eCollection 2019.
DNA-based non-invasive prenatal testing (NIPT) using maternal blood constitutes an emerging technology for the detection of Down syndrome (DS). The aim of the study was to conduct a cost-effectiveness analysis to evaluate the economic costs and health implications of the introduction of NIPT based on cell-free foetal DNA analysis through different screening strategies for the detection of DS.
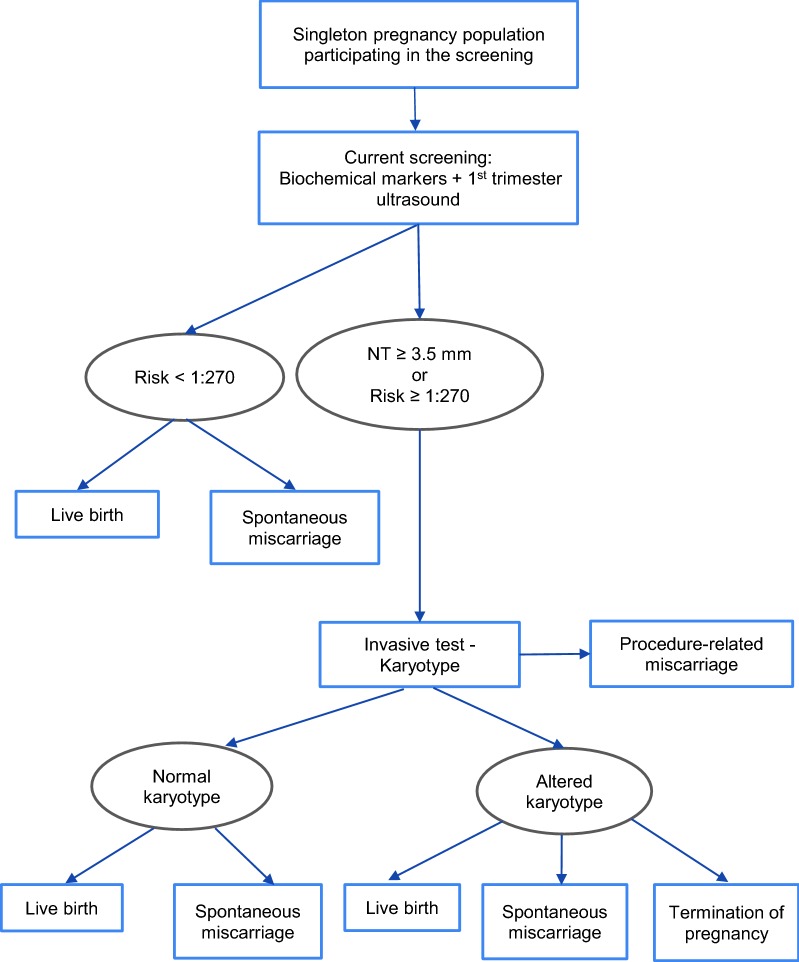
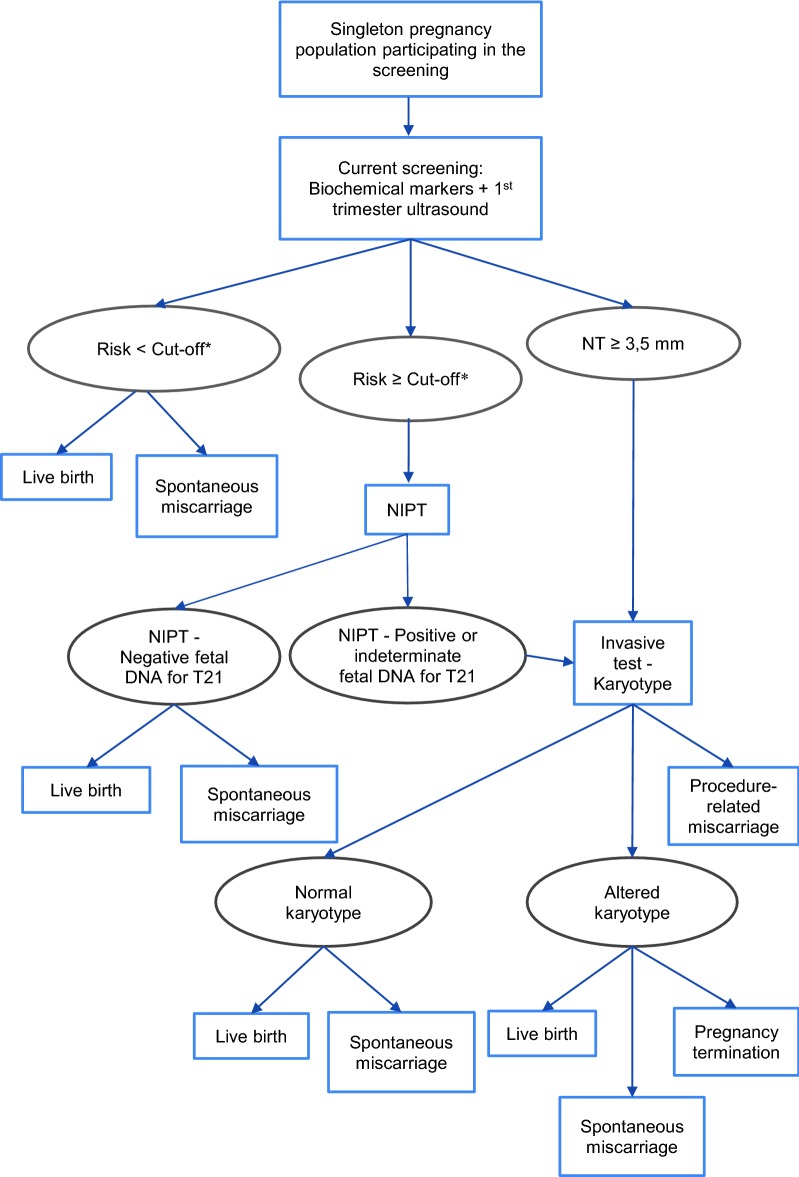
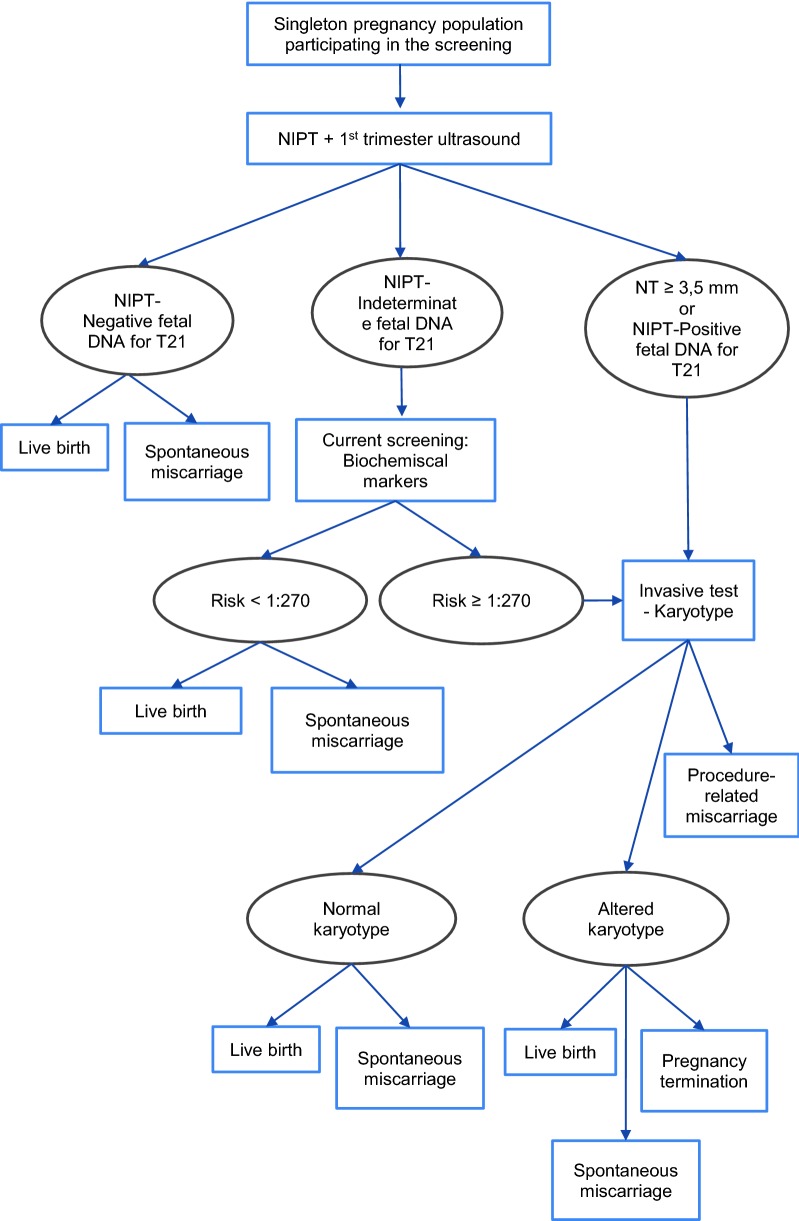
An analytical short-term decision model was developed, from the payer´s perspective (Spanish National Health Service). The main outcome measure was the number of DS cases detected. Secondary measures included associated miscarriages, women undergoing current screening, women undergoing NIPT, positive NIPT and invasive procedures performed. The study setting was the Spanish National Health Service. Three strategies were compared: (a) first- and second-trimester screening (current screening); (b) NIPT as contingent testing; and (c) NIPT as first-line testing. Modelling was based on a hypothetical cohort of 100,000 Spanish pregnant women. Population data were obtained from the database of the Basque Antenatal Screening Programme. Deterministic sensitivity analyses were performed to assess variations in the cost of NIPT, screening risk cut-off, screening uptake-rate and rate of failure of NIPT.
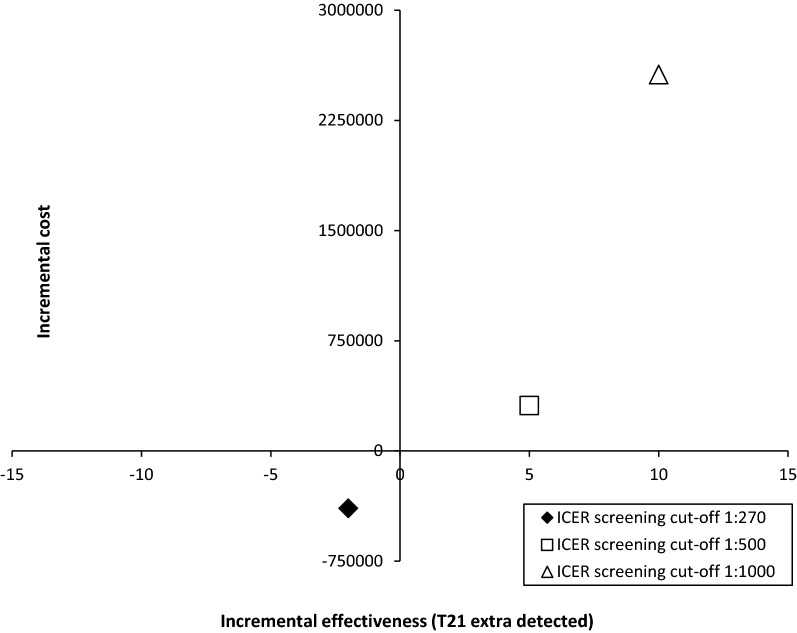
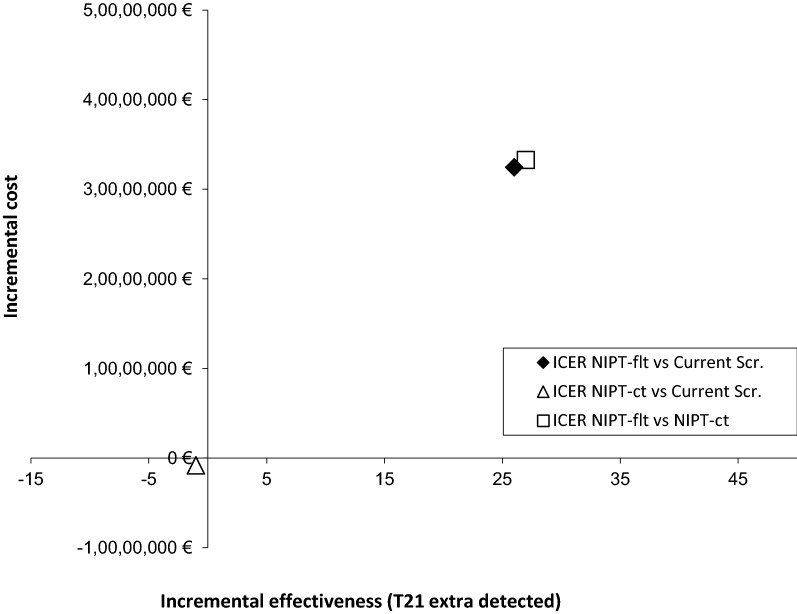
NIPT as contingent testing (strategy b) led to fewer miscarriages following invasive procedures and a slight reduction in the number of DS cases detected compared to current screening. However, lowering the screening cut-off to ≥ 1:500 would improve the overall effectiveness of NIPT as contingent testing, increasing the number of DS cases detected and decreasing foetal losses as compared to the current screening, despite there would be an extra-cost of 3.5%. When NIPT was used as first-line testing (strategy c), the screening would be more effective but also more expensive, with incremental cost-effectiveness ratios (ICERs) per additional case of DS detected of €1,299,763 and €1,232,763, compared with strategies a and b, respectively. Results were sensitive to the different parameters considered in the analysis.
Both, as first-line testing and as contingent testing when screening cut-off was lowered ≥ 1:500, NIPT would lead to more favourable outcomes as compared to the current screening (both in terms of DS cases detected and miscarriages avoided), but at a greater cost.
利用孕妇血液进行基于DNA的无创产前检测(NIPT)是一种用于检测唐氏综合征(DS)的新兴技术。本研究的目的是进行成本效益分析,以评估通过不同的唐氏综合征检测筛查策略引入基于游离胎儿DNA分析的无创产前检测的经济成本和对健康的影响。
从支付方(西班牙国家卫生服务局)的角度开发了一个短期分析决策模型。主要结局指标是检测到的唐氏综合征病例数。次要指标包括相关的流产、接受当前筛查的妇女、接受无创产前检测的妇女、无创产前检测呈阳性的情况以及进行的侵入性检查。研究背景是西班牙国家卫生服务局。比较了三种策略:(a)孕早期和孕中期筛查(当前筛查);(b)将无创产前检测作为补充检测;(c)将无创产前检测作为一线检测。建模基于100, 000名西班牙孕妇的假设队列。人口数据来自巴斯克产前筛查计划的数据库。进行了确定性敏感性分析,以评估无创产前检测成本、筛查风险临界值、筛查接受率和无创产前检测失败率的变化。
与当前筛查相比,将无创产前检测作为补充检测(策略b)可减少侵入性检查后的流产次数,且检测到的唐氏综合征病例数略有减少。然而,将筛查临界值降低至≥1:500可提高无创产前检测作为补充检测的总体有效性,与当前筛查相比,检测到的唐氏综合征病例数增加,胎儿丢失减少,尽管会额外增加3.5%的成本。当将无创产前检测用作一线检测(策略c)时,筛查将更有效,但成本也更高,与策略a和b相比,每多检测出一例唐氏综合征病例的增量成本效益比(ICER)分别为1,299,763欧元和1,232,763欧元。结果对分析中考虑的不同参数敏感。
无论是作为一线检测,还是在筛查临界值降低至≥1:500时作为补充检测,与当前筛查相比,无创产前检测都会带来更有利的结果(在检测到的唐氏综合征病例数和避免流产方面),但成本更高。