Department of Clinical and Experimental Epilepsy, University College London Institute of Neurology, London, UK.
Magnetic Resonance Imaging Unit, Epilepsy Society, London, UK.
Epilepsia. 2019 Apr;60(4):718-729. doi: 10.1111/epi.14689. Epub 2019 Mar 14.
The processes underlying sudden unexpected death in epilepsy (SUDEP) remain elusive, but centrally mediated cardiovascular or respiratory collapse is suspected. Volume changes in brain areas mediating recovery from extreme cardiorespiratory challenges may indicate failure mechanisms and allow prospective identification of SUDEP risk.
We retrospectively imaged SUDEP cases (n = 25), patients comparable for age, sex, epilepsy syndrome, localization, and disease duration who were high-risk (n = 25) or low-risk (n = 23), and age- and sex-matched healthy controls (n = 25) with identical high-resolution T1-weighted scans. Regional gray matter volume, determined by voxel-based morphometry, and segmentation-derived structure sizes were compared across groups, controlling for total intracranial volume, age, and sex.
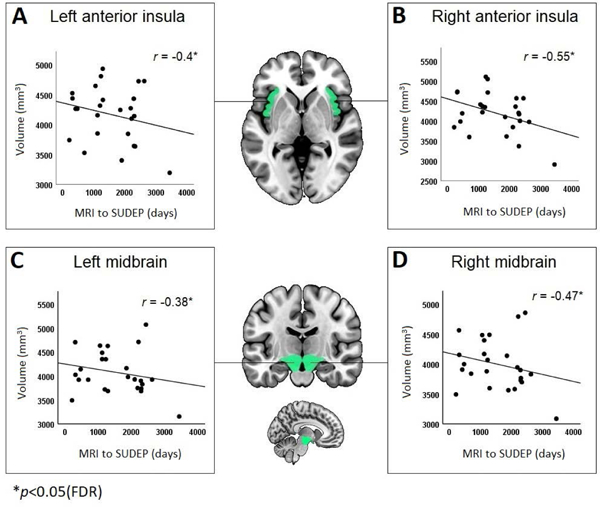
Substantial bilateral gray matter loss appeared in SUDEP cases in the medial and lateral cerebellum. This was less prominent in high-risk subjects and absent in low-risk subjects. The periaqueductal gray, left posterior and medial thalamus, left hippocampus, and bilateral posterior cingulate also showed volume loss in SUDEP. High-risk subjects showed left thalamic volume reductions to a lesser extent. Bilateral amygdala, entorhinal, and parahippocampal volumes increased in SUDEP and high-risk patients, with the subcallosal cortex enlarged in SUDEP only. Disease duration correlated negatively with parahippocampal volume. Volumes of the bilateral anterior insula and midbrain in SUDEP cases were larger the closer to SUDEP from magnetic resonance imaging.
SUDEP victims show significant tissue loss in areas essential for cardiorespiratory recovery and enhanced volumes in areas that trigger hypotension or impede respiratory patterning. Those changes may shed light on SUDEP pathogenesis and prospectively detect patterns identifying those at risk.
癫痫猝死(SUDEP)的发病机制仍不清楚,但怀疑与中枢介导的心血管或呼吸衰竭有关。调节从极端心肺挑战中恢复的脑区的体积变化可能表明失败机制,并允许前瞻性识别 SUDEP 风险。
我们回顾性地对 SUDEP 病例(n=25)、年龄、性别、癫痫综合征、定位和疾病持续时间可比的高危(n=25)或低危(n=23)患者以及年龄和性别匹配的健康对照(n=25)进行了成像,所有患者均接受了相同的高分辨率 T1 加权扫描。通过基于体素的形态计量学确定的区域灰质体积和分割衍生的结构大小在各组之间进行了比较,控制了总颅内体积、年龄和性别。
SUDEP 病例的内侧和外侧小脑出现了大量双侧灰质丢失。高危组的情况不太明显,低危组则没有。中脑导水管周围灰质、左侧丘脑后内侧、左侧海马体和双侧后扣带回在 SUDEP 中也显示出体积损失。高危组的左丘脑体积减少程度较轻。双侧杏仁核、内嗅皮质和海马旁回在 SUDEP 和高危患者中体积增加,只有 SUDEP 患者的胼胝体下皮质增大。疾病持续时间与海马旁回体积呈负相关。SUDEP 病例双侧前岛叶和中脑体积越大,距磁共振成像上的 SUDEP 越近。
SUDEP 受害者在对心肺恢复至关重要的区域显示出明显的组织丢失,而在引发低血压或阻碍呼吸模式的区域则显示出增强的体积。这些变化可能有助于阐明 SUDEP 的发病机制,并前瞻性地检测出识别高危人群的模式。