Chantal BIYA International Reference Centre for research on HIV/AIDS prevention and management, Yaoundé, Cameroon.
Faculty of Medicine and Biomedical Sciences, University of Yaoundé I, Yaoundé, Cameroon.
BMC Infect Dis. 2019 Mar 12;19(1):246. doi: 10.1186/s12879-019-3871-0.
With the phase-out of stavudine (d4T), change to first-line regimens with zidovudine (AZT) or tenofovir (TDF) in resource-limited settings (RLS) might increase risks of cross-resistance to nucleos(t) ide reverse transcriptase inhibitors (NRTI). This would restrict the scope of switching to the World Health Organisation (WHO)-recommended standard second-line combinations (SLC) without HIV drug resistance (HIVDR)-testing in routine clinical practice.
An observational study was conducted among 101 Cameroonian patients (55.4% male, median [IQR] age 34 [10-41] years) failing first-line antiretroviral therapy (ART) in 2016, and stratified into three groups according to NRTIs exposure: exposure to both thymidine analogues AZT "and" D4T (group-A, n = 55); exposure to both TDF and AZT "or" D4T (group-B, n = 22); exposure solely to D4T (group-C, n = 24). Protease-reverse transcriptase HIVDR was interpreted using the HIVdb penalty scores (≥60: high-resistance; 20-59: intermediate-resistance; < 20: susceptible). The acceptable threshold for potential-efficacy was set at 80%.
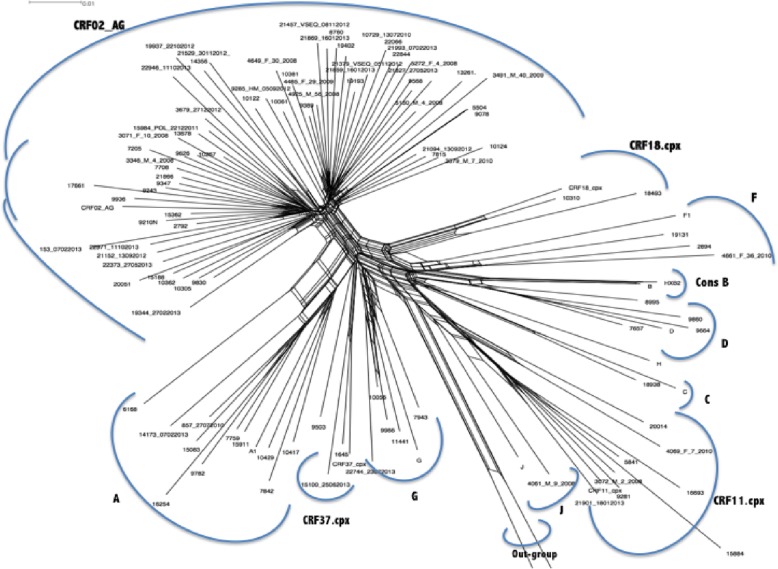
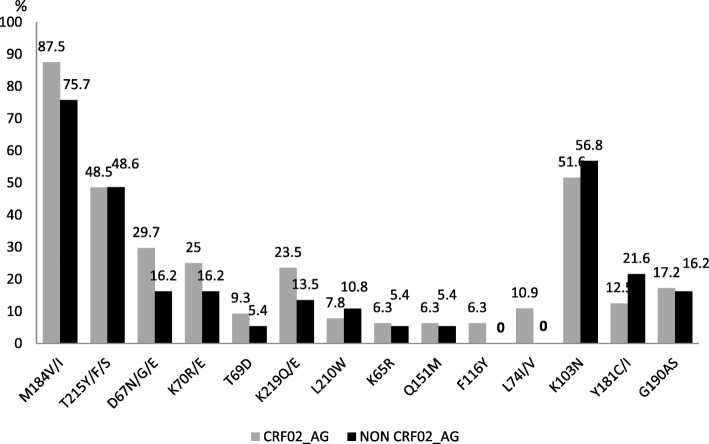
The median [IQR] CD4, viral RNA, and time on ART, were respectively 129 [29-466] cells/μl, 71,630 [19,041-368,000] copies/ml, and 4 [2-5] years. Overall HIVDR-level was 89.11% (90/101), with 83.2% harbouring M184 V (high-level 3TC/FTC-resistance) and only 1.98% (2/101) major HIVDR-mutations to ritonavir-boosted protease-inhibitors (PI/r). Thymidine-analogue mutations (TAMs)-1 [T215FY (46.53%), M41 L (22.77%), L210 W (8.91%)], with cross-resistance to AZT and TDF, were higher compared to TAMs-2 [D67N (21.78%), K70R (19.80%), K219QE (18.81%)]. As expected, K65R was related with TDF-exposure: 0% (0/55) in group-A, 22.72% (5/22) group-B, 4.17% (1/24) group-C (p = 0.0013). The potential-efficacy of AZT vs. TDF was respectively 43.64% (24/55) vs. 70.91% (39/55) in group-A (p = 0.0038); 63.64% (14/22) vs. 68.28% (15/22) in group-B (p = 1.0000); and 37.50% (9/24) vs. 83.33% (20/24) in group-C (p = 0.0032). CRF02_AG was the prevailing subtype (63.40%), followed by CRF11.cpx (8.91%), A (7.92%), G (5.94%); without any significant effect of the subtype-distribution on HIVDR (92.2% in CRF02_AG vs. 83.8% in non-AG; p = 0.204).
First-line ART-failure exhibits high-level NRTI-resistance, with potential lower-efficacy of AZT compared to TDF. Significantly, using our 80% efficacy-threshold, only patients without NRTI-substitution on first-line could effectively switch to SLC following the WHO-approach. Patients with multiple NRTI-substitutions (exposed to both thymidine-analogues and TDF) on first-line ART would require HIVDR-testing to select active NRTIs for SLC.
在资源有限的环境下(RLS),停用司他夫定(d4T)并转换为一线方案中的齐多夫定(AZT)或替诺福韦(TDF)可能会增加对核苷(酸)逆转录酶抑制剂(NRTI)交叉耐药的风险。这将限制在常规临床实践中不进行 HIV 耐药性(HIVDR)检测的情况下,转换为世界卫生组织(WHO)推荐的标准二线联合治疗方案(SLC)的范围。
在 2016 年,对 101 名在一线抗逆转录病毒治疗(ART)中失败的喀麦隆患者(55.4%为男性,中位[IQR]年龄 34[10-41]岁)进行了一项观察性研究,并根据 NRTI 暴露情况分为三组:同时暴露于两种胸苷类似物 AZT“和”D4T(组 A,n=55);同时暴露于 TDF 和 AZT“或”D4T(组 B,n=22);仅暴露于 D4T(组 C,n=24)。使用 HIVdb 罚分(≥60:高度耐药;20-59:中度耐药;<20:敏感)来解释蛋白酶-逆转录酶 HIVDR。潜在疗效的可接受阈值设定为 80%。
中位[IQR]CD4、病毒 RNA 和 ART 时间分别为 129[29-466]个/μl、71630[19041-368000]个拷贝/ml 和 4[2-5]年。总体 HIVDR 水平为 89.11%(90/101),83.2%携带 M184V(高水平 3TC/FTC 耐药),仅有 1.98%(2/101)发生主要 HIVDR 突变对利托那韦增效蛋白酶抑制剂(PI/r)。胸苷类似物突变(TAMs)-1[T215FY(46.53%)、M41L(22.77%)、L210W(8.91%)]与 AZT 和 TDF 的交叉耐药性较高,而 TAMs-2[D67N(21.78%)、K70R(19.80%)、K219QE(18.81%)]则较低。如预期的那样,K65R 与 TDF 暴露相关:组 A 中为 0%(0/55),组 B 中为 22.72%(5/22),组 C 中为 4.17%(1/24)(p=0.0013)。AZT 与 TDF 的潜在疗效在组 A 中分别为 43.64%(24/55)和 70.91%(39/55)(p=0.0038);在组 B 中分别为 63.64%(14/22)和 68.28%(15/22)(p=1.0000);在组 C 中分别为 37.50%(9/24)和 83.33%(20/24)(p=0.0032)。CRF02_AG 是主要的亚型(63.40%),其次是 CRF11.cpx(8.91%)、A(7.92%)和 G(5.94%);但亚型分布对 HIVDR 没有显著影响(CRF02_AG 中为 92.2%,非 AG 中为 83.8%;p=0.204)。
一线治疗失败表现出高水平的 NRTI 耐药性,与 TDF 相比,AZT 的潜在疗效较低。重要的是,使用我们的 80%疗效阈值,只有未在一线方案中进行 NRTI 替代的患者才能按照 WHO 方法有效地转换为 SLC。一线 ART 中已进行多种 NRTI 替代(同时暴露于胸苷类似物和 TDF)的患者需要进行 HIVDR 检测,以选择 SLC 中有效的 NRTI。