Arthur Davison Children's Hospital, Ndola, Zambia.
Tropical Diseases Research Center, Ndola, Zambia.
PLoS One. 2020 Aug 17;15(8):e0236156. doi: 10.1371/journal.pone.0236156. eCollection 2020.
HIV drug resistance (HIVDR) poses a threat to the HIV epidemic control in Zambia especially in sub-populations such as the 15-24 years where there is poor virological suppression. Understanding the prevalence and patterns of HIVDR in this population (15-24 years) will contribute to defining effective antiretroviral therapy (ART) regimens, improving clinical decision making, and supporting behavioral change interventions needed to achieve HIV epidemic control.
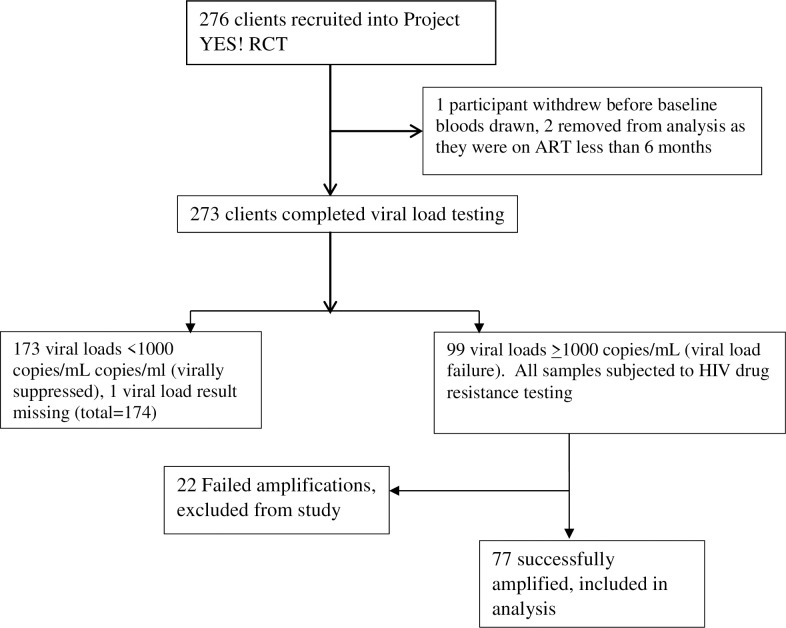
A cross-sectional analysis of study enrollment data from the Project YES! Youth Engaging for Success randomized controlled trial was conducted. Participants were 15 to 24 years old, who knew their HIV status, and had been on ART for at least 6 months. All participants completed a survey and underwent viral load (VL) testing. Participants with viral failure (VL ≥1,000 copies/mL) underwent HIVDR testing which included analysis of mutations in the protease and reverse transcriptase genes.
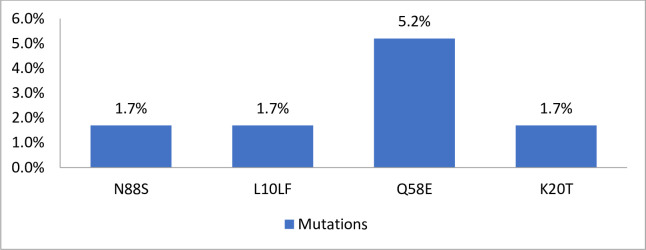
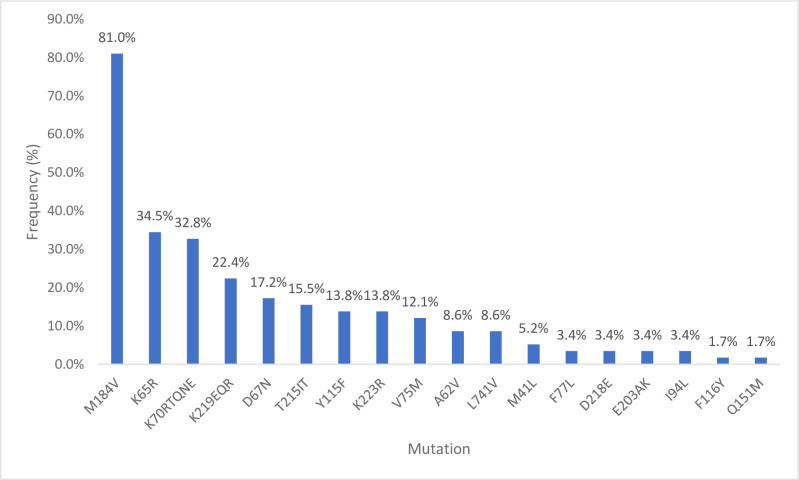
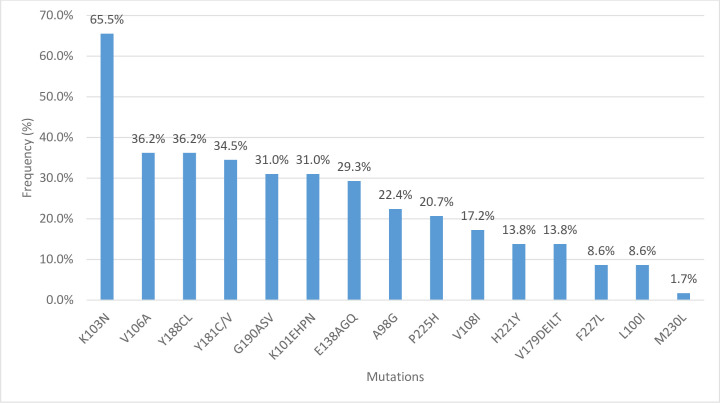
A total of 99 out of 273 analyzed participants receiving ART had VL failure, of whom 77 had successful HIVDR amplification and analysis. Out of the 77, 75% (58) had at least one drug resistant mutation, among which 83% (48/58) required a drug change. Among the 58 with HIVDR mutations, the prevalence of at least one HIVDR mutation to nucleoside reverse transcriptase inhibitors (NRTIs), non-nucleoside reverse transcriptase inhibitors (NNRTIs) and protease inhibitors (PIs) were 81%, 65.5% and 1.7%. The mutation M184V which confers resistance to NRTI drugs of lamivudine (3TC) and emtricitabine (FTC) was the most common (81%) among NRTI associated mutations followed by K65R (34.5%) which is associated with both tenofovir disoproxil fumarate (TDF) and tenofovir alafenamide fumarate (TAF) resistance. Thymidine analogue mutations (TAMs) which confer resistance primarily to zidovudine (AZT), stavudine (d4T) and other NRTIs were observed at 32.8%. Common TAMs were K70RTQNE (32.8%), K219QE (22.4%), D67N (17.2%) and T215IT (15.5%). The most common NNRTI associated mutation was the K103N (65.5%) which confers resistance to both efavirenz (EFV) and nevirapine (NVP). There was a relatively high occurrence of other NNRTI mutations V106A (36.2%), as well as Y188C (36.2%) and Y181C (36.2%) which confer resistance to etravirine.
There is a high prevalence of HIVDR including TAMs despite majority of these patients (90.48%) being on AZT or d4T sparing first line ART among the youth. Emergence of these mutations including the NNRTI associated mutations (Y181C and Y188C) may compromise future second- and third-line regimens in the absence of routine HIVDR testing. HIVDR monitoring at start of ART or at first-line failure can better inform clinical decision making and ART programing.
艾滋病病毒耐药性(HIVDR)对赞比亚的艾滋病疫情控制构成威胁,特别是在青少年 15-24 岁人群中,病毒学抑制效果不佳。了解该人群(15-24 岁)中 HIVDR 的流行情况和模式,将有助于确定有效的抗逆转录病毒治疗(ART)方案,改善临床决策,并支持实现艾滋病疫情控制所需的行为改变干预措施。
对 Project YES!青年成功参与随机对照试验的研究入组数据进行了横断面分析。参与者年龄在 15 至 24 岁之间,他们知晓自己的 HIV 状况,并已接受至少 6 个月的 ART 治疗。所有参与者都完成了一项调查,并接受了病毒载量(VL)检测。病毒载量失败(VL≥1000 拷贝/mL)的参与者进行了 HIVDR 检测,包括分析蛋白酶和逆转录酶基因中的突变。
在接受 ART 的 273 名分析参与者中,共有 99 人出现病毒载量失败,其中 77 人成功进行了 HIVDR 扩增和分析。在这 77 人中,75%(58 人)有至少一种耐药突变,其中 83%(48/58)需要药物更换。在 58 名具有 HIVDR 突变的患者中,核苷逆转录酶抑制剂(NRTIs)、非核苷逆转录酶抑制剂(NNRTIs)和蛋白酶抑制剂(PIs)至少有 1 种耐药突变的发生率分别为 81%、65.5%和 1.7%。M184V 突变是最常见的 NRTI 相关突变(81%),可导致拉米夫定(3TC)和恩曲他滨(FTC)等 NRTI 药物耐药,其次是 K65R(34.5%)突变,它与替诺福韦二吡呋酯(TDF)和替诺福韦艾拉酚胺富马酸盐(TAF)耐药有关。主要导致齐多夫定(AZT)、司他夫定(d4T)和其他 NRTIs 耐药的胸苷类似物突变(TAMs)发生率为 32.8%。常见的 TAMs 为 K70RTQNE(32.8%)、K219QE(22.4%)、D67N(17.2%)和 T215IT(15.5%)。最常见的 NNRTI 相关突变是 K103N(65.5%),它可导致依非韦伦(EFV)和奈韦拉平(NVP)耐药。其他 NNRTI 突变 V106A(36.2%)、Y188C(36.2%)和 Y181C(36.2%)的发生率也相对较高,这些突变可导致依曲韦林耐药。
尽管大多数青少年(90.48%)在一线治疗中使用 AZT 或 d4T 作为节省药物的方案,但仍存在很高的 HIVDR 流行率,包括 TAMs。这些突变的出现,包括 NNRTI 相关突变(Y181C 和 Y188C),可能会在没有常规 HIVDR 检测的情况下,破坏未来的二线和三线治疗方案。在开始 ART 或一线治疗失败时进行 HIVDR 监测,可以更好地为临床决策和 ART 规划提供信息。