Zhou Zhongbao, Cui Yuanshan, Wu Jitao, Ding Rui, Cai Tong, Gao Zhenli
Binzhou Medical University, Yantai, Shandong, China.
Department of Urology, The Affiliated Yantai Yuhuangding Hospital of Qingdao University, Yantai, NO. 20 East Yuhuangding Road, Yantai, 264000, Shandong, China.
BMC Urol. 2019 Mar 11;19(1):17. doi: 10.1186/s12894-019-0446-8.
We performed a meta-analysis to confirm the efficacy and safety of the combination of tamsulosin plus dutasteride compared with tamsulosin monotherapy in treating benign prostatic hyperplasia (BPH) during a treatment cycle of at least 1 year.
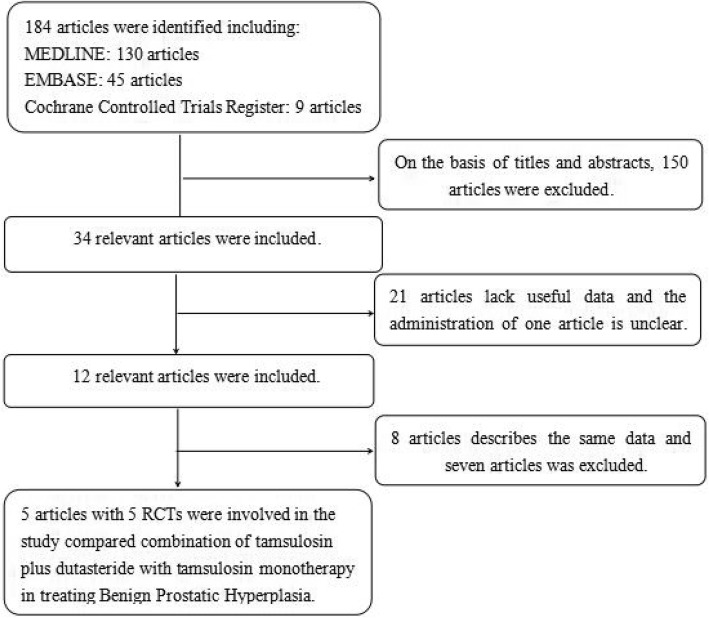
Randomized controlled trials were searched by using MEDLINE, EMBASE, and the Cochrane Controlled Trials Register. Systematic review was carried out using the Preferred Reporting Items for Systematic Reviews and Meta-analyses. The data was evaluated and statistically analyzed by using RevMan version 5.3.0.
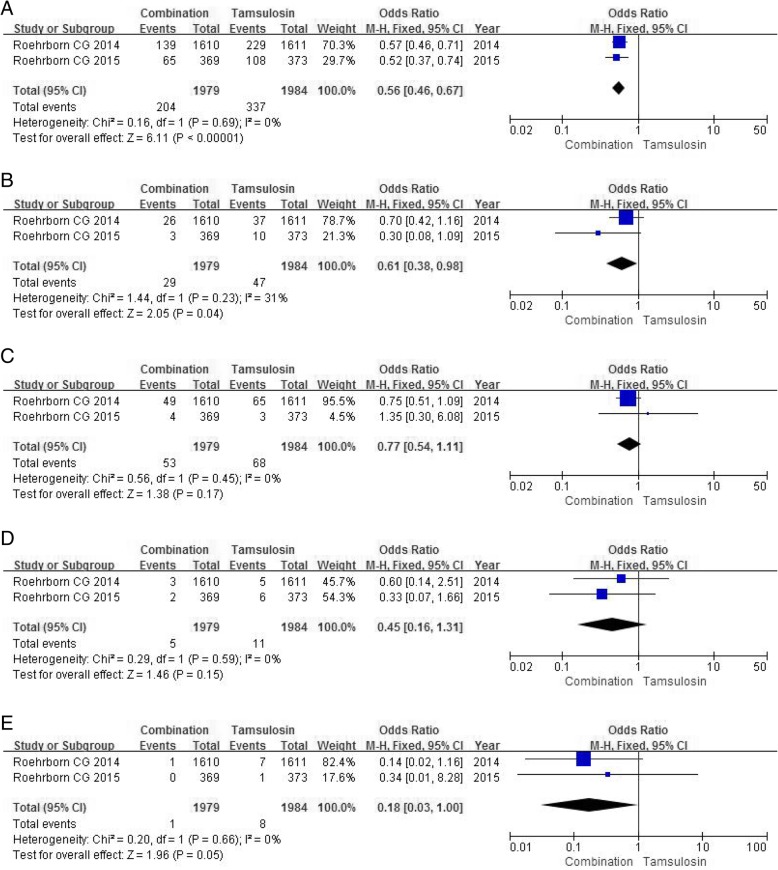
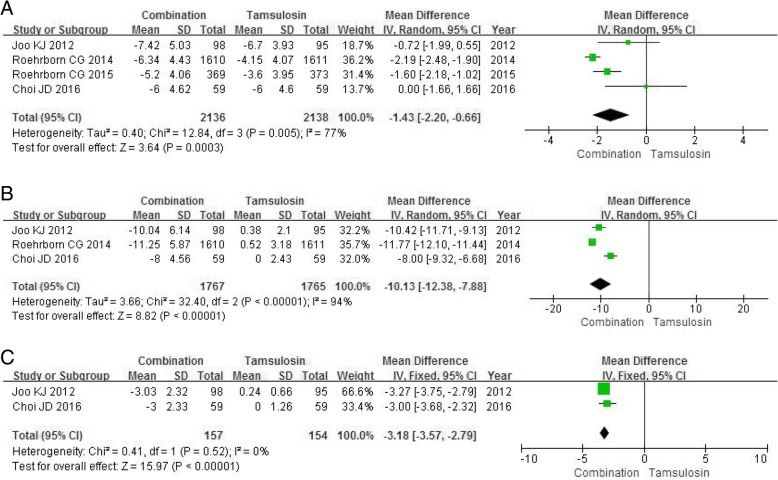
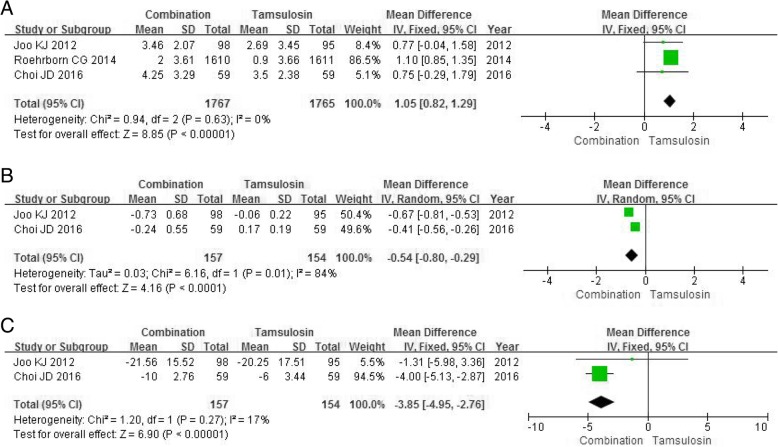
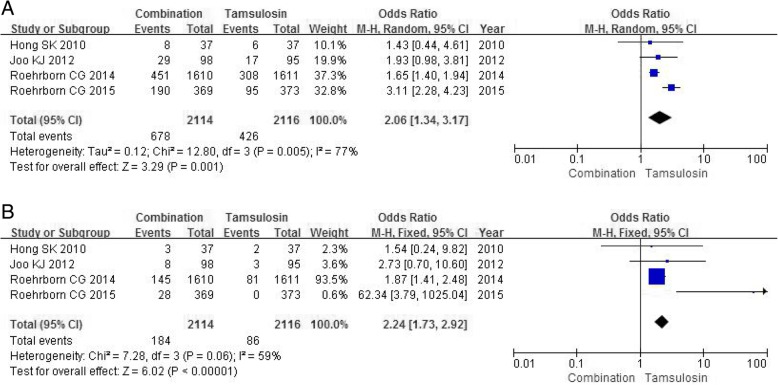
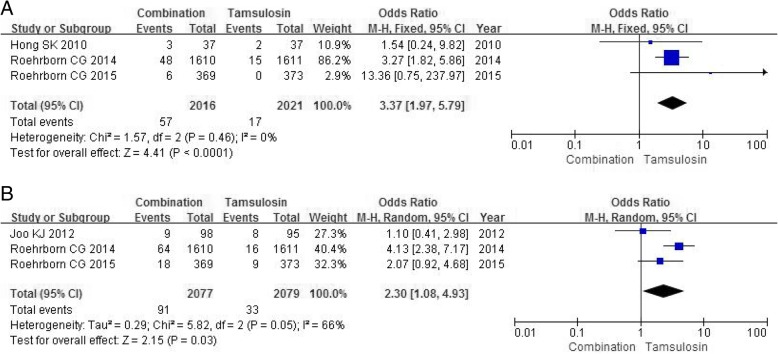
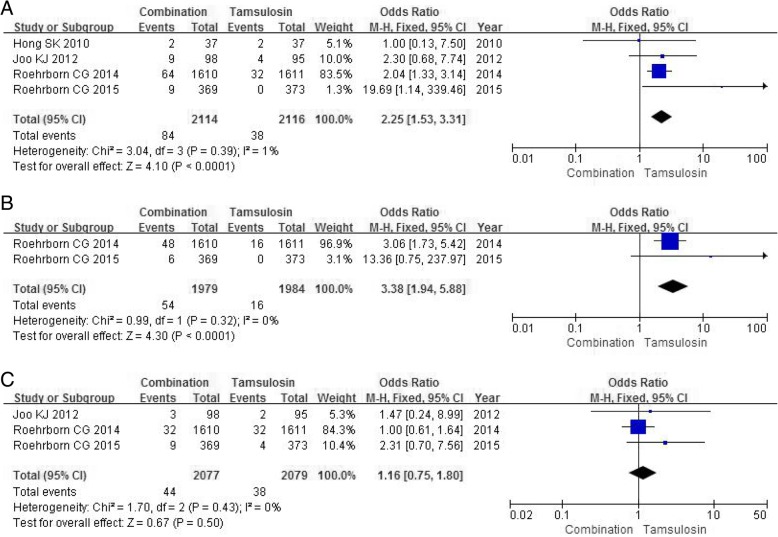
Five studies including 4348 patients were studied. The analysis found that the combination group was significantly greater effect in international prostate symptom score (mean difference [MD], - 1.43; 95% confidence interval [CI], - 2.20 to - 0.66; P = 0.0003), prostate volume (MD, - 10.13; 95% CI, - 12.38 to - 7.88; P < 0.00001), transitional zone volume (MD, - 3.18; 95% CI, - 3.57 to - 2.79; P<0.0001), maximum urine flow rate (MD, 1.05; 95% CI, 0.82 to 1.29; P < 0.00001), prostate specific antigen (MD, - 0.54; 95% CI, - 0.80 to - 0.29; P < 0.0001) and post-void residual volume (MD, - 3.85; 95% CI, - 4.95 to - 2.76; P < 0.00001) compared with the tamsulosin group. In terms of safety, including adverse events (odds ratio [OR], 2.06; 95% CI, 1.34 to 3.17; P = 0.001), erectile dysfunction (OR, 2.24; 95% CI, 1.73 to 2.92; P < 0.00001), ejaculation disorder (OR, 3.37; 95% CI, 1.97 to 5.79; P < 0.0001), retrograde ejaculation (OR, 2.30; 95% CI, 1.08 to 4.93; P = 0.03), decreased libido (OR, 2.25; 95% CI, 1.53 to 3.31; P < 0.0001) and loss of libido (OR, 3.38; 95% CI, 1.94 to 5.88; P<0.0001), the combination group showed poor tolerance than the tamsulosin group with the exception of dizziness (OR, 1.16; 95% CI, 0.75 to 1.80; P = 0.50). The combination group significantly reduced the risk of clinical progression than the tamsulosin group especially in incidence of BPH-related symptom progression (OR, 0.56; 95% CI, 0.46 to 0.67; P < 0.00001) and acute urinary retention (OR, 0.61; 95% CI, 0.38 to 0.98; P = 0.04).
The combination of tamsulosin plus dutasteride provides a preferable therapeutic effect for BPH with a higher incidence of sexual side effects, but combination-therapy can markedly reduce risk of BPH-related symptom progression and acute urinary retention relative to tamsulosin monotherapy.
我们进行了一项荟萃分析,以确认在至少1年的治疗周期中,坦索罗辛联合度他雄胺与坦索罗辛单药治疗良性前列腺增生(BPH)的疗效和安全性。
通过检索MEDLINE、EMBASE和Cochrane对照试验注册库来查找随机对照试验。使用系统评价和荟萃分析的首选报告项目进行系统评价。使用RevMan 5.3.0版本对数据进行评估和统计分析。
共纳入5项研究,涉及4348例患者。分析发现,与坦索罗辛组相比,联合治疗组在国际前列腺症状评分(平均差值[MD],-1.43;95%置信区间[CI],-2.20至-0.66;P = 0.0003)、前列腺体积(MD,-10.13;95% CI,-12.38至-7.88;P < 0.00001)、移行区体积(MD,-3.18;95% CI,-3.57至-2.79;P < 0.0001)、最大尿流率(MD,1.05;95% CI,0.82至1.29;P < 0.00001)、前列腺特异性抗原(MD,-0.54;I95% CI,-0.80至-0.29;P < 0.0001)和残余尿量(MD,-3.85;95% CI,-4.95至-2.76;P < 0.00001)方面有显著更好的效果。在安全性方面,包括不良事件(比值比[OR],2.06;95% CI,1.34至3.17;P = 0.001)、勃起功能障碍(OR,2.24;95% CI,1.73至2.92;P < 0.00001)、射精障碍(OR,3.37;95% CI,1.97至5.79;P < 0.0001)、逆行射精(OR,2.30;95% CI,1.08至4.93;P = 0.03)、性欲减退(OR,2.25;95% CI,1.53至3.31;P < 0.0001)和性欲丧失(OR,3.38;95% CI,1.94至5.88;P < 0.0001),联合治疗组的耐受性比坦索罗辛组差,但头晕除外(OR,1.16;95% CI,0.75至1.80;P = 0.50)。联合治疗组比坦索罗辛组显著降低了临床进展的风险,尤其是在BPH相关症状进展的发生率(OR,0.56;95% CI,0.46至0.67;P < 0.00001)和急性尿潴留(OR,0.61;95% CI,0.38至0.98;P = 0.04)方面。
坦索罗辛联合度他雄胺对BPH有较好的治疗效果,但性副作用发生率较高,不过联合治疗相对于坦索罗辛单药治疗可显著降低BPH相关症状进展和急性尿潴留的风险。