Follia Laura, Ferrero Giulio, Mandili Giorgia, Beccuti Marco, Giordano Daniele, Spadi Rosella, Satolli Maria Antonietta, Evangelista Andrea, Katayama Hiroyuki, Hong Wang, Momin Amin A, Capello Michela, Hanash Samir M, Novelli Francesco, Cordero Francesca
Center for Experimental Research and Medical Studies, Azienda Universitaria Ospedaliera Città della Salute e della Scienza di Torino, Turin, Italy.
Department of Molecular Biotechnology and Health Sciences, University of Turin, Turin, Italy.
Front Oncol. 2019 Feb 27;9:115. doi: 10.3389/fonc.2019.00115. eCollection 2019.
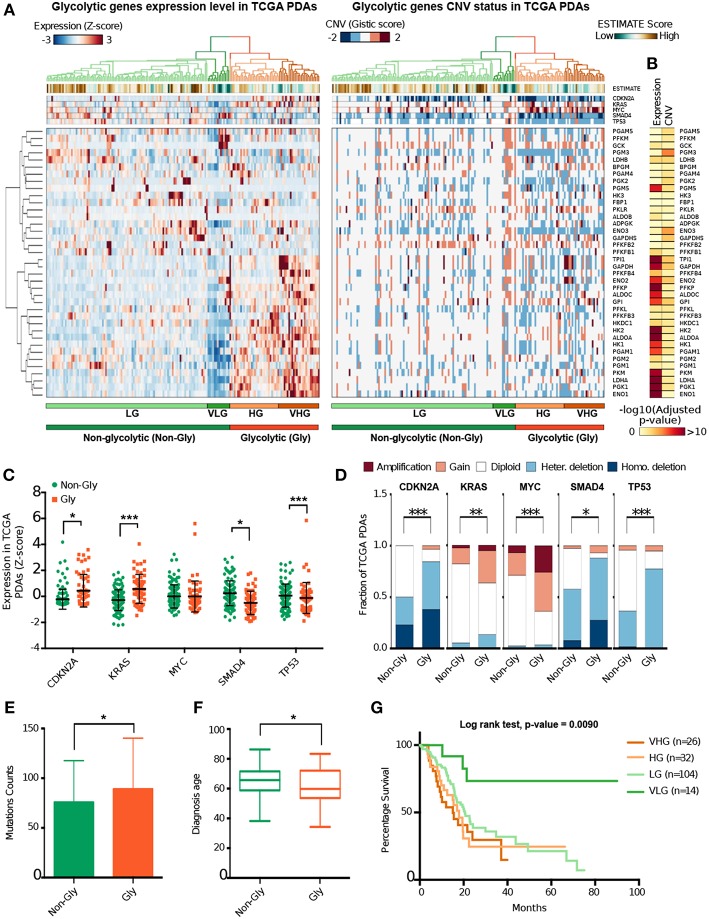
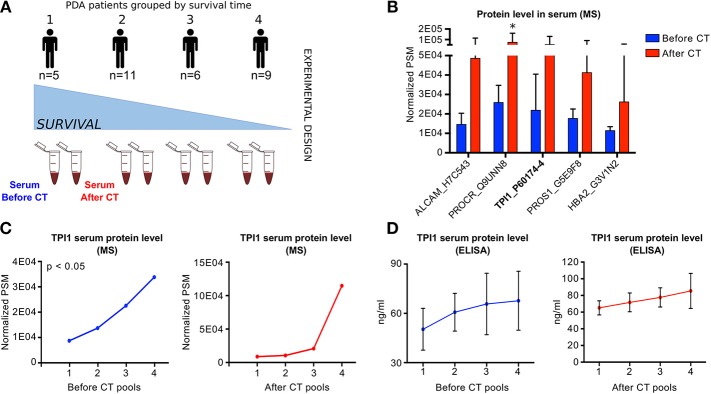
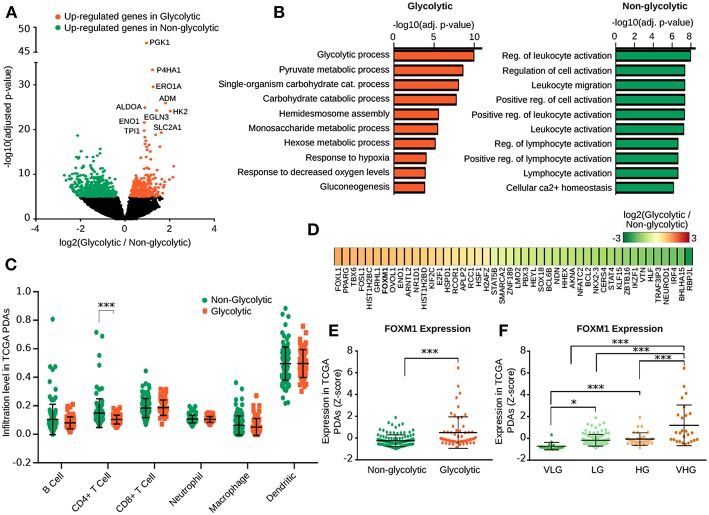
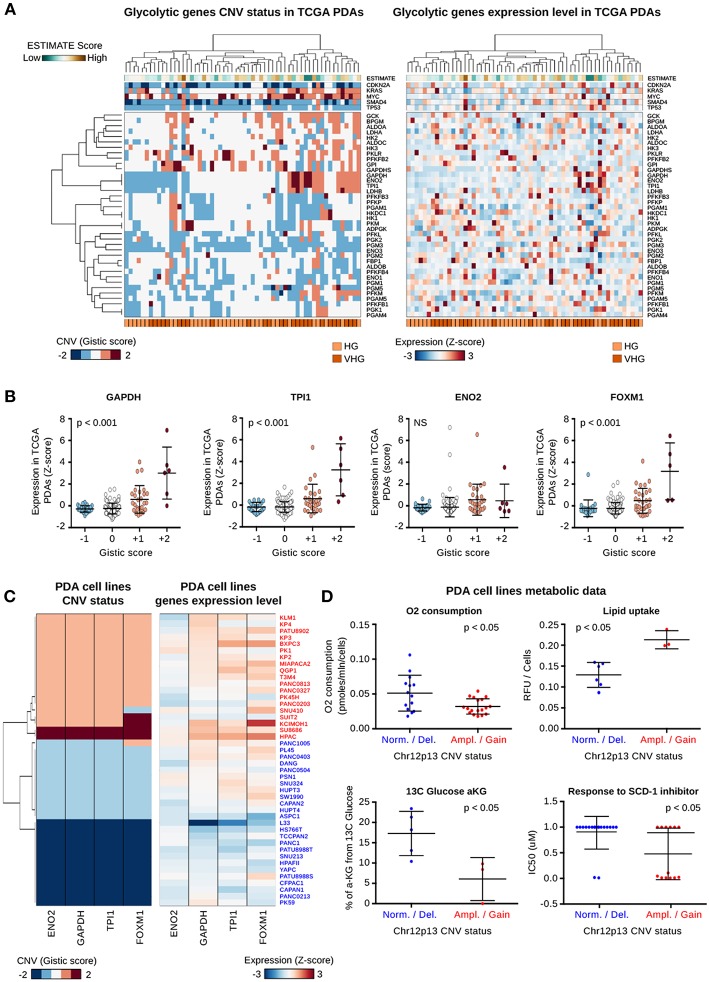
Most of the patients with Pancreatic Ductal Adenocarcinoma (PDA) are not eligible for a curative surgical resection. For this reason there is an urgent need for personalized therapies. PDA is the result of complex interactions between tumor molecular profile and metabolites produced by its microenvironment. Despite recent studies identified PDA molecular subtypes, its metabolic classification is still lacking. We applied an integrative analysis on transcriptomic and genomic data of glycolytic genes in PDA. Data were collected from public datasets and molecular glycolytic subtypes were defined using hierarchical clustering. The grade of purity of the cancer samples was assessed estimating the different amount of stromal and immunological infiltrate among the identified PDA subtypes. Analyses of metabolomic data from a subset of PDA cell lines allowed us to identify the different metabolites produced by the metabolic subtypes. Sera of a cohort of 31 PDA patients were analyzed using Q-TOF mass spectrometer to measure the amount of metabolic circulating proteins present before and after chemotherapy. Our integrative analysis of glycolytic genes identified two glycolytic and two non-glycolytic metabolic PDA subtypes. Glycolytic patients develop disease earlier, have poor prognosis, low immune-infiltrated tumors, and are characterized by a gain in chr12p13 genomic region. This gain results in the over-expression of , and . PDA cell lines with the gain of chr12p13 are characterized by an higher lipid uptake and sensitivity to drug targeting the fatty acid metabolism. Our sera proteomic analysis confirms that TPI1 serum levels increase in poor prognosis gemcitabine-treated patients. We identify four metabolic PDA subtypes with different prognosis outcomes which may have pivotal role in setting personalized treatments. Moreover, our data suggest TPI1 as putative prognostic PDA biomarker.
大多数胰腺导管腺癌(PDA)患者不符合根治性手术切除的条件。因此,迫切需要个性化治疗。PDA是肿瘤分子特征与其微环境产生的代谢物之间复杂相互作用的结果。尽管最近的研究确定了PDA分子亚型,但其代谢分类仍然缺乏。我们对PDA中糖酵解基因的转录组和基因组数据进行了综合分析。数据从公共数据集收集,并使用层次聚类定义分子糖酵解亚型。通过估计已鉴定的PDA亚型中基质和免疫浸润的不同量来评估癌症样本的纯度等级。对一部分PDA细胞系的代谢组学数据进行分析,使我们能够鉴定出代谢亚型产生的不同代谢物。使用Q-TOF质谱仪分析了31名PDA患者队列的血清,以测量化疗前后代谢循环蛋白的量。我们对糖酵解基因的综合分析确定了两种糖酵解和两种非糖酵解代谢的PDA亚型。糖酵解型患者疾病进展较早,预后较差,肿瘤免疫浸润低,其特征是12号染色体p13区域扩增。这种扩增导致 、 和 的过度表达。具有12号染色体p13扩增的PDA细胞系的特征是脂质摄取增加以及对靶向脂肪酸代谢的药物敏感。我们的血清蛋白质组学分析证实,在吉西他滨治疗的预后较差的患者中,TPI1血清水平升高。我们鉴定出四种具有不同预后结果的代谢性PDA亚型,它们可能在制定个性化治疗中起关键作用。此外,我们的数据表明TPI1作为PDA的潜在预后生物标志物。