Department of Respiratory and Critical Care Medicine, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences, Peking Union Medical College, Beijing, China.
Department of Pathology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences, Peking Union Medical College, Beijing, China.
EBioMedicine. 2019 Apr;42:304-310. doi: 10.1016/j.ebiom.2019.03.023. Epub 2019 Mar 14.
Tyrosine kinase inhibitors (TKIs) are clinically effective in non-small cell lung cancer (NSCLC) patients harbouring epidermal growth factor receptor (EGFR) oncogene mutations. Genetic factors, other than EGFR sensitive mutations, that allow prognosis of TKI treatment remain undefined.
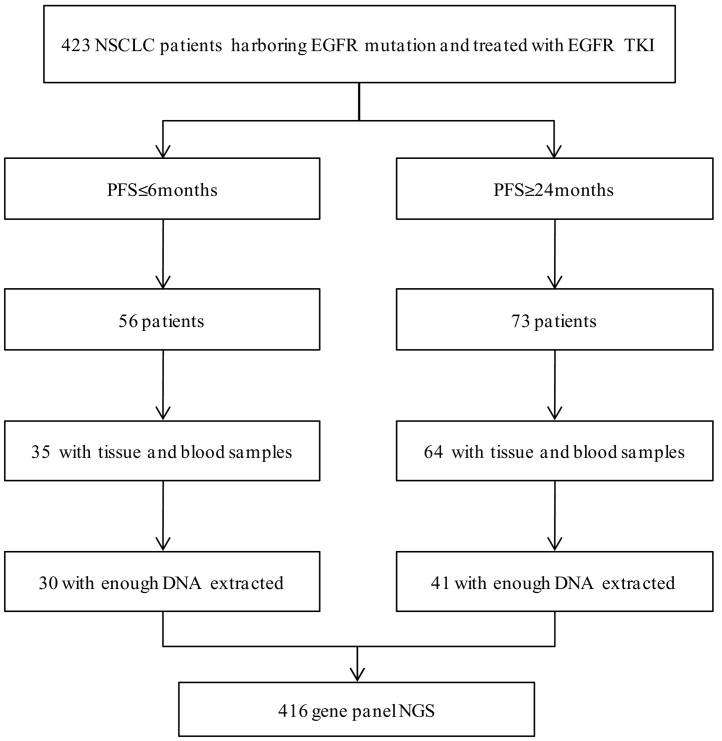
We retrospectively screened 423 consecutive patients with advanced NSCLC and EGFR 19del or 21L858R mutations. A total of 71 patients whose progression-free survivals (PFS) were shorter than 6 months or longer than 24 months were included and stratified into separate groups. Genetic background discrepancy was analysed in the two groups using next generation sequencing (NGS).
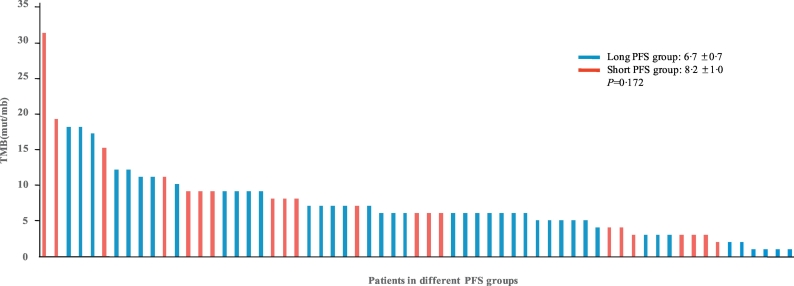
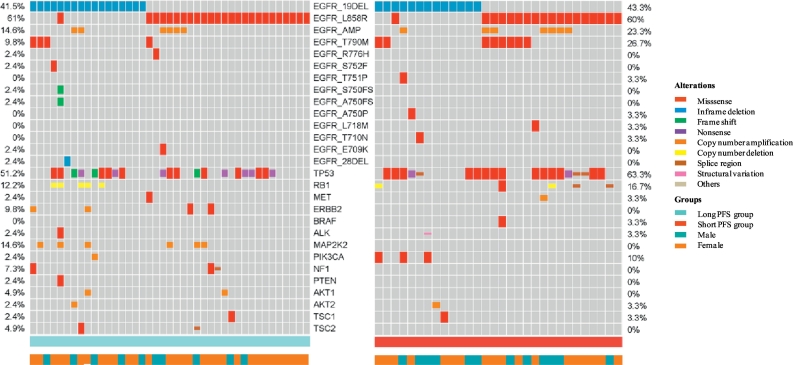
Sensitive EGFR mutations of 19del or 21L858R were detected by NGS in all patients; the 21L858R mutation was the major type. The most frequent accompanying somatic mutations were TP53, RB1, MAP2K. ALK fusion, MET amplification, and BRAF V600E were found only in the short PFS group. Concurrent pretreament T790 M mutation was found in both groups, but was proportionally higher in the short PFS group. In the short PFS group, patients had significantly more driver gene mutations than in long PFS group (P = 0·018). The numbers of concomitant somatic mutations, EGFR pathway-related mutations, and tumor mutation burden (TMB) were not significantly different between the two groups.
Co-occuring driver gene mutations were negative predictive factors of TKI therapy in EGFR-mutated patients. This study highlights the importance of exploring co-occuring genomic alterations before initiation of EGFR-TKIs.
酪氨酸激酶抑制剂(TKI)在携带表皮生长因子受体(EGFR)基因突变的非小细胞肺癌(NSCLC)患者中具有临床疗效。除 EGFR 敏感突变外,允许预测 TKI 治疗效果的遗传因素仍未确定。
我们回顾性筛选了 423 例晚期 NSCLC 患者和 EGFR 19del 或 21L858R 突变患者。共纳入 71 例无进展生存期(PFS)短于 6 个月或长于 24 个月的患者,并将其分为两组。使用下一代测序(NGS)分析两组之间的遗传背景差异。
所有患者均通过 NGS 检测到 19del 或 21L858R 的敏感 EGFR 突变,21L858R 突变是主要类型。最常见的伴随体细胞突变是 TP53、RB1、MAP2K。ALK 融合、MET 扩增和 BRAF V600E 仅在 PFS 短组中发现。两组均发现了同时性预处理 T790M 突变,但在 PFS 短组中比例更高。在 PFS 短组中,患者的驱动基因突变明显多于 PFS 长组(P=0.018)。两组之间同时发生的体细胞突变、EGFR 通路相关突变和肿瘤突变负担(TMB)没有显著差异。
同时发生的驱动基因突变是 EGFR 突变患者 TKI 治疗的阴性预测因素。本研究强调了在开始 EGFR-TKIs 治疗前探索同时发生的基因组改变的重要性。