1 Department of Neurology Charité-Universitätsmedizin Berlin, Campus Benjamin Franklin Berlin Germany.
6 Department of Neurology Medical Park Berlin Humboldtmühle Berlin Germany.
J Am Heart Assoc. 2019 Mar 19;8(6):e011729. doi: 10.1161/JAHA.118.011729.
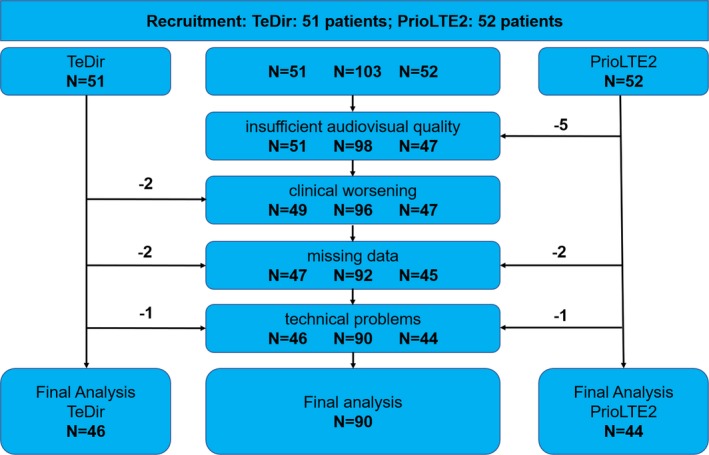
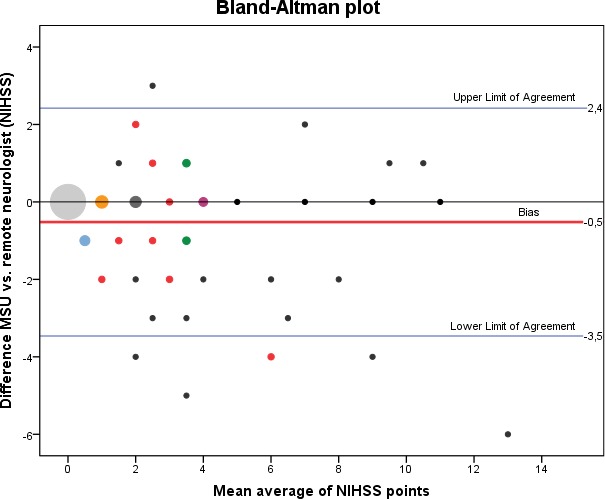
Background Mobile stroke units ( MSU s), equipped with an integrated computed tomography scanner, can shorten time to thrombolytic treatment and may improve outcome in patients with acute ischemic stroke. Original (German) MSU s are staffed by neurologists trained as emergency physicians, but patient assessment and treatment decisions by a remote neurologist may offer an alternative to neurologists aboard MSU . Methods and Results Remote neurologists examined and assessed emergency patients treated aboard the MSU in Berlin, Germany. Audiovisual quality was rated by the remote neurologist from 1 (excellent) to 6 (insufficient), and duration of video examinations was assessed. We analyzed interrater reliability of diagnoses, scores on the National Institutes of Health Stroke Scale and treatment decisions (intravenous thrombolysis) between the MSU neurologist and the remote neurologist. We included 90 of 103 emergency assessments (13 patients were excluded because of either failed connection, technical problems, clinical worsening during teleconsultation, or missing data in documentation) in this study. The remote neurologist rated audiovisual quality with a median grade for audio quality of 3 (satisfactory) and for video quality of 2 (good). Mean time for completion of teleconsultations was about 19±5 minutes. The interrater reliabilities between the onboard and remote neurologist were high for diagnoses (Cohen's κ=0.86), National Institutes of Health Stroke Scale sum scores (intraclass correlation coefficient, 0.87) and treatment decisions (16 treatment decisions agreed versus 2 disagreed; Cohen's κ=0.93). Conclusions Remote assessment and treatment decisions of emergency patients are technically feasible with satisfactory audiovisual quality. Agreement on diagnoses, neurological examinations, and treatment decisions between onboard and remote neurologists was high.
配备集成计算机断层扫描(CT)扫描仪的移动卒中单元(MSU)可以缩短溶栓治疗时间,并可能改善急性缺血性脑卒中患者的预后。原(德)MSU 由接受过急诊医师培训的神经科医生组成,但远程神经科医生对 MSU 上患者的评估和治疗决策可能是 MSU 上神经科医生的替代方案。
远程神经科医生检查和评估了德国柏林 MSU 上的急救患者。远程神经科医生对视听质量进行了 1(优秀)至 6(不足)的评分,并评估了视频检查的持续时间。我们分析了 MSU 神经科医生和远程神经科医生之间的诊断、美国国立卫生研究院卒中量表评分和治疗决策(静脉溶栓)的诊断间可靠性。本研究共纳入了 103 例急救评估中的 90 例(13 例因连接失败、技术问题、远程会诊期间病情恶化或记录中缺失数据而被排除)。远程神经科医生对音频质量的平均评分中位数为 3(满意),对视频质量的平均评分中位数为 2(良好)。远程会诊完成时间平均约为 19±5 分钟。MSU 上的神经科医生和远程神经科医生之间的诊断间可靠性较高(Cohen's κ=0.86)、美国国立卫生研究院卒中量表总分(组内相关系数,0.87)和治疗决策(16 次治疗决策一致,2 次不一致;Cohen's κ=0.93)。
远程评估和急救患者的治疗决策在技术上是可行的,具有令人满意的视听质量。MSU 上的神经科医生和远程神经科医生在诊断、神经科检查和治疗决策方面具有较高的一致性。