Siedlecki Andrew M, Isbel Nicole, Vande Walle Johan, James Eggleston Jennifer, Cohen David J
Brigham and Women's Hospital, Boston, Massachusetts, USA.
The University of Queensland and Princess Alexandra Hospital, Brisbane, Australia.
Kidney Int Rep. 2018 Dec 3;4(3):434-446. doi: 10.1016/j.ekir.2018.11.010. eCollection 2019 Mar.
Recurrence of atypical hemolytic uremic syndrome (aHUS) in renal allografts is common, leading to dialysis and graft failure. Pretransplant versus posttransplant initiation of eculizumab treatment in patients with aHUS has not been rigorously investigated. We hypothesized eculizumab pretransplant would reduce dialysis incidence posttransplant.
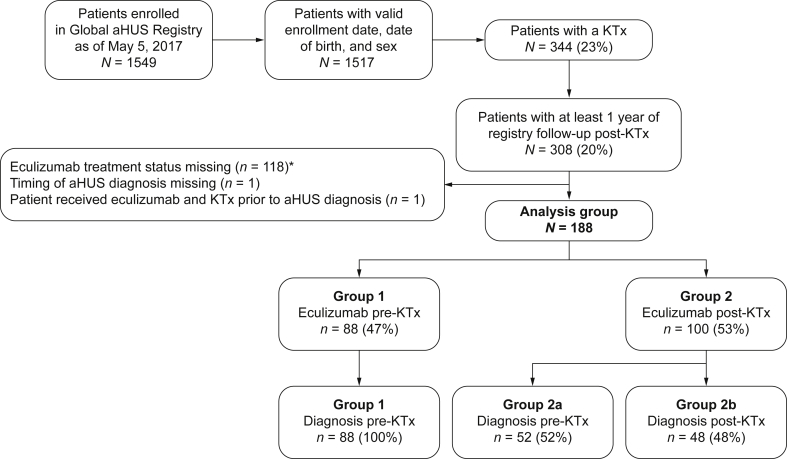
Of patients enrolled in the Global aHUS Registry ( = 1549), 344 had ≥1 kidney transplant. Of these, 188 had received eculizumab. Eighty-eight patients (47%) were diagnosed with aHUS and received eculizumab before, and during, their most recent transplant (group 1). A total of 100 patients (53%; group 2) initiated eculizumab posttransplantation. This second group was subdivided into those diagnosed with aHUS before ( = 52; group 2a) or after ( = 48; group 2b) their most recent transplant.
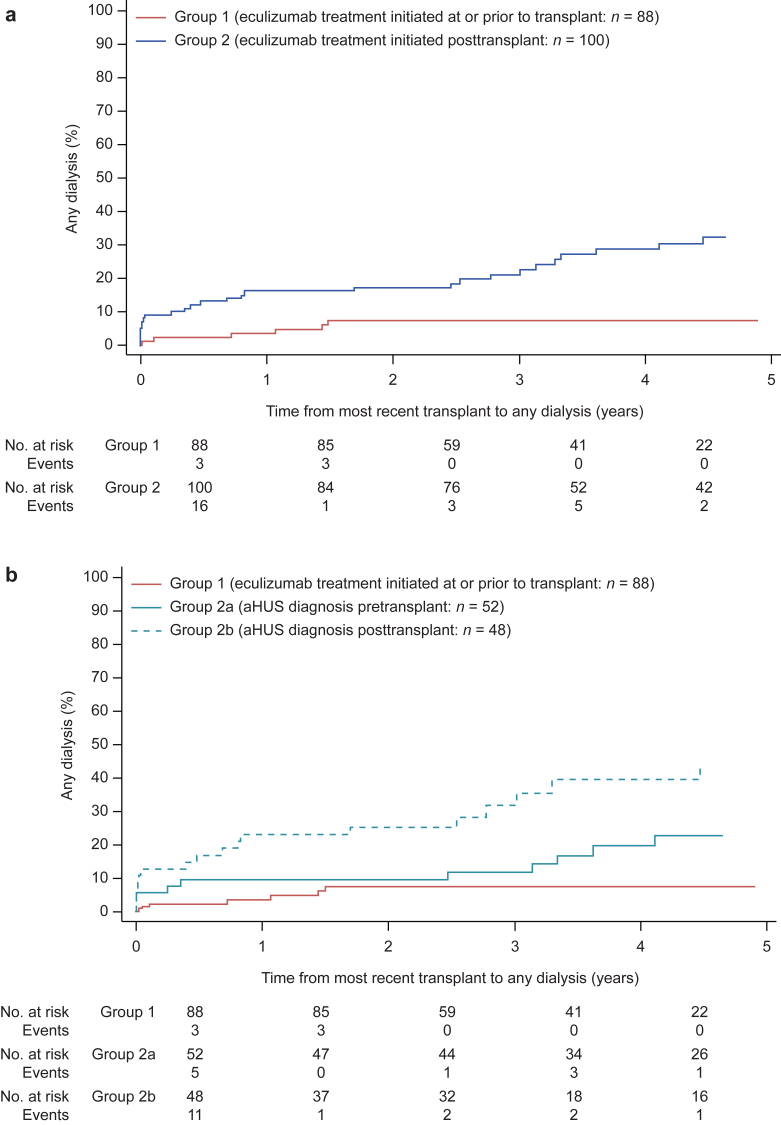
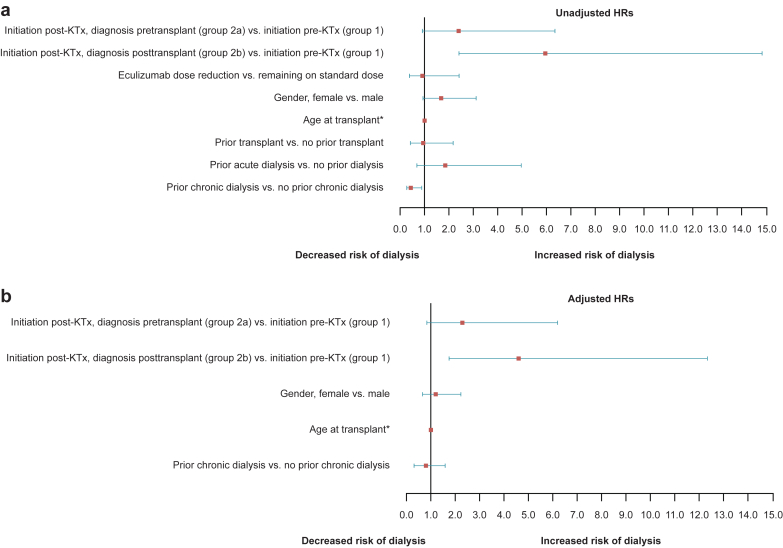
Within 5 years of transplantation, 47 patients required dialysis; the risk of dialysis after transplantation was significantly increased in group 2b (hazard ratio [HR] 4.6; confidence interval [CI] 1.7-12.4) but not 2a (HR 2.3; CI 0.9-6.2). Graft function within 6 months of transplantation was significantly better in group 1 (median estimated glomerular filtration rate of 60.6 ml/min per 1.73 m) compared with 31.5 and 9.6 ml/min per 1.73 m in groups 2a ( = 0.004) and 2b ( = 0.0001), respectively. One meningococcal infection (resolved with treatment) and 3 deaths (deemed unrelated to eculizumab) were reported.
Outcomes for transplant patients with aHUS treated with eculizumab were improved compared with previous reports of patients with aHUS not treated with eculizumab. Our findings suggest delayed aHUS diagnosis and therefore treatment is associated with an increased risk of dialysis posttransplantation and reduced allograft function.
肾移植中不典型溶血尿毒综合征(aHUS)复发很常见,会导致透析和移植肾失功。对于aHUS患者,在移植前与移植后开始使用依库珠单抗治疗尚未进行严格研究。我们推测移植前使用依库珠单抗可降低移植后透析发生率。
在全球aHUS注册研究(n = 1549)纳入的患者中,344例进行了≥1次肾移植。其中,188例接受了依库珠单抗治疗。88例患者(47%)在其最近一次移植前及移植期间被诊断为aHUS并接受了依库珠单抗治疗(第1组)。共有100例患者(53%;第2组)在移植后开始使用依库珠单抗。第二组又细分为在其最近一次移植前(n = 52;第2a组)或移植后(n = 48;第2b组)被诊断为aHUS的患者。
在移植后5年内,47例患者需要透析;第2b组移植后透析风险显著增加(风险比[HR] 4.6;置信区间[CI] 1.7 - 12.4),而第2a组未增加(HR 2.3;CI 0.9 - 6.2)。移植后6个月内,第1组的移植肾功能明显更好(估计肾小球滤过率中位数为每1.73 m² 60.6 ml/min),相比之下,第2a组(P = 0.004)和第2b组(P = 0.0001)分别为每1.73 m² 31.5 ml/min和9.6 ml/min。报告了1例脑膜炎球菌感染(治疗后痊愈)和3例死亡(认为与依库珠单抗无关)。
与既往未接受依库珠单抗治疗的aHUS患者报告相比,接受依库珠单抗治疗的aHUS移植患者的结局有所改善。我们的研究结果表明,aHUS诊断延迟进而治疗延迟与移植后透析风险增加及移植肾功能降低有关。