Menne Jan, Delmas Yahsou, Fakhouri Fadi, Kincaid John F, Licht Christoph, Minetti Enrico E, Mix Chris, Provôt François, Rondeau Eric, Sheerin Neil S, Wang Jimmy, Weekers Laurent E, Greenbaum Larry A
Klinik für Nieren- und Hochdruckerkrankungen, Hannover, Germany.
CHU de Bordeaux, Bordeaux, France.
Clin Kidney J. 2018 May 16;12(2):196-205. doi: 10.1093/ckj/sfy035. eCollection 2019 Apr.
Eculizumab, a terminal complement inhibitor, is approved for atypical haemolytic uraemic syndrome (aHUS) to inhibit complement-mediated thrombotic microangiopathy (TMA).
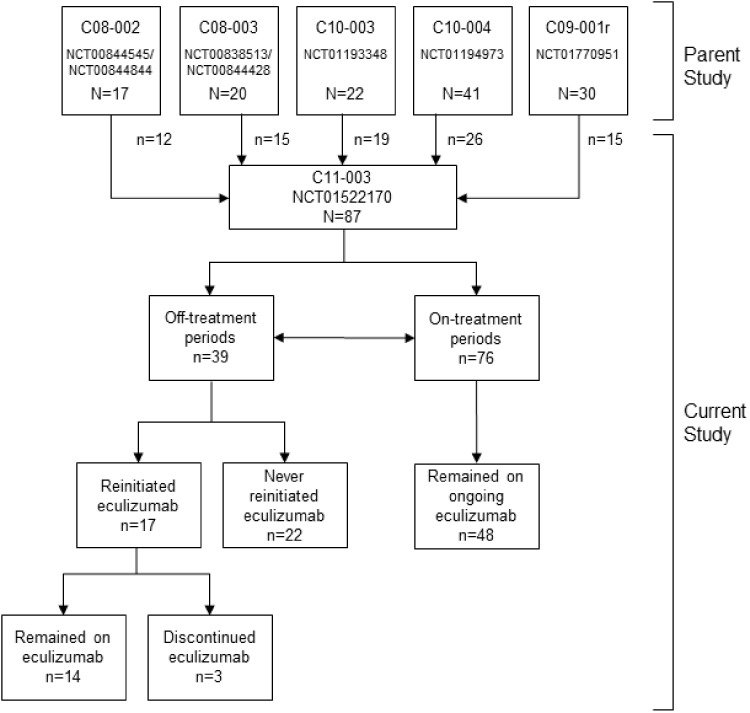
In five parent studies, eculizumab effectively prevented TMA and improved renal and haematologic outcomes in patients with aHUS; therefore, these patients could enrol in this long-term, prospective, observational and multicentre study. The primary endpoint was the TMA manifestation rate off and on eculizumab post-parent study. analyses evaluated rates during labelled versus non-labelled dosing regimens, and in those with versus without identified complement abnormalities. Serious targeted treatment-emergent adverse events (TEAEs) were evaluated.
Of 87 patients in the current study, 39 and 76 had off- and on-treatment periods, respectively; 17 (44%) with off periods reinitiated eculizumab. TMA manifestation rate per 100 patient-years was 19.9 off and 7.3 on treatment [hazard ratio (HR), 4.7; P = 0.0008]; rates were highest off treatment and lowest during labelled regimens. TMA manifestations with hospitalizations/serious AEs occurred more frequently off versus on treatment. TMA rates were higher among patients with identified complement abnormalities (HR, 4.5; P = 0.0082). Serious targeted TEAEs occurred at similar rates off and on treatment.
As expected, patients with aHUS have increased risk of TMA manifestations after discontinuation of eculizumab or in the setting of non-labelled eculizumab dosing. Collectively, results show that maintaining eculizumab treatment minimizes risk of TMA, particularly in patients with identified complement abnormalities. Future studies are needed to further characterize TMA and longer term outcomes on labelled or non-labelled eculizumab regimens and after discontinuation of treatment.
依库珠单抗是一种终末补体抑制剂,已被批准用于治疗非典型溶血性尿毒症综合征(aHUS),以抑制补体介导的血栓性微血管病(TMA)。
在五项母研究中,依库珠单抗有效预防了aHUS患者的TMA,并改善了其肾脏和血液学结局;因此,这些患者可以参加这项长期、前瞻性、观察性多中心研究。主要终点是母研究后依库珠单抗停药和用药期间的TMA表现率。分析评估了标记给药方案与非标记给药方案期间以及有和没有已确定补体异常的患者中的发生率。对严重的目标治疗出现的不良事件(TEAE)进行了评估。
在本研究的87例患者中,分别有39例和76例有停药期和治疗期;17例(44%)停药期患者重新开始使用依库珠单抗。每100患者年的TMA表现率在停药期为19.9,在治疗期为7.3[风险比(HR),4.7;P = 0.0008];停药期发生率最高,标记给药方案期间最低。伴有住院/严重不良事件的TMA表现停药期比治疗期更频繁出现。已确定补体异常的患者中TMA发生率更高(HR,4.5;P = 0.0082)。严重的目标TEAE在停药期和治疗期的发生率相似。
正如预期的那样,aHUS患者在停用依库珠单抗后或在非标记依库珠单抗给药情况下出现TMA表现的风险增加。总体而言,结果表明维持依库珠单抗治疗可将TMA风险降至最低,尤其是在已确定补体异常的患者中。未来需要进一步研究以更全面地描述TMA以及标记或非标记依库珠单抗方案和停药后的长期结局。