Department of Nutritional Sciences and Toxicology, University of California, Berkeley, USA.
Department of Medicine, Oregon Health and Science University, Portland, USA.
J Cachexia Sarcopenia Muscle. 2019 Feb;10(1):14-21. doi: 10.1002/jcsm.12390. Epub 2019 Mar 21.
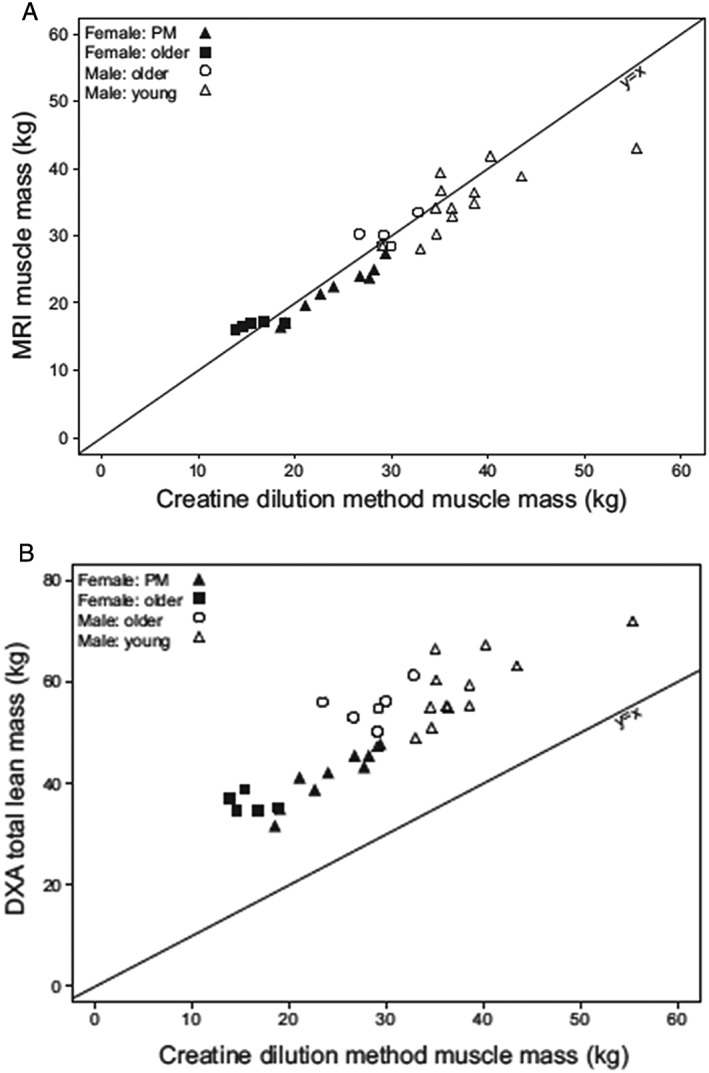
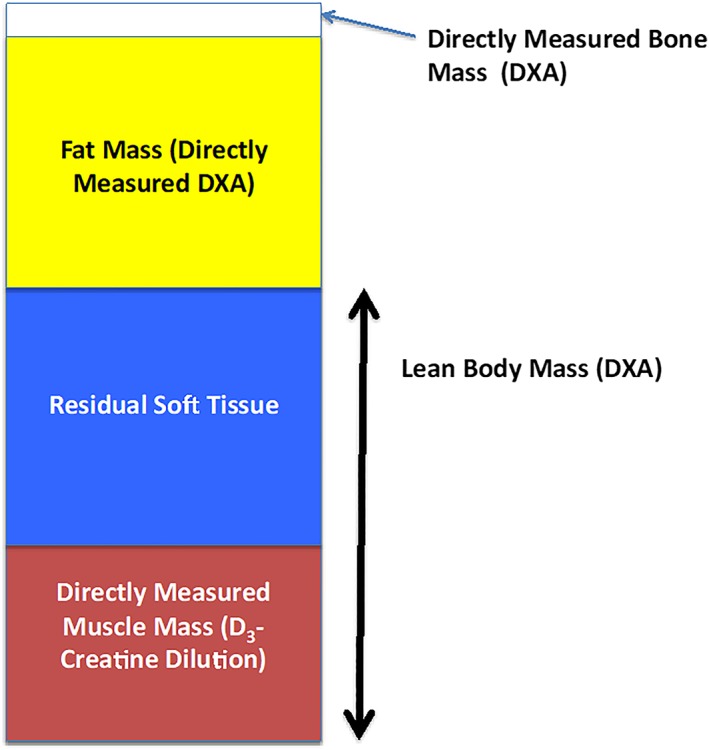
Sarcopenia has been described as the age-associated decrease in skeletal muscle mass. However, virtually every study of sarcopenia has measured lean body mass (LBM) or fat free mass (FFM) rather than muscle mass, specifically. In a number of published sarcopenia studies, LBM or FFM is referred to as muscle mass, leading to an incorrect assumption that measuring LBM or FFM is an accurate measure of muscle mass. As a result, the data on the effects of changes in LBM or FFM in older populations on outcomes such as functional capacity, disability, and risk of injurious falls have been inconsistent resulting in the conclusion that muscle mass is only weakly related to these outcomes. We review and describe the assumptions for the most commonly used measurements of body composition. Dual-energy X-ray absorptiometry (DXA) has become an increasingly common tool for the assessment of LBM or FFM and appendicular lean mass as a surrogate, but inaccurate, measurement of muscle mass. Other previously used methods (total body water, bioelectric impedance, and imaging) also have significant limitations. D -Creatine (D -Cr) dilution provides a direct and accurate measurement of creatine pool size and skeletal muscle mass. In a recent study in older men (MrOS cohort), D -Cr muscle mass was associated with functional capacity and risk of injurious falls and disability, while assessments of LBM or appendicular lean mass by DXA were only weakly or not associated with these outcomes. Inaccurate measurements of muscle mass by DXA and other methods have led to inconsistent results and potentially erroneous conclusions about the importance of skeletal muscle mass in health and disease. The assessment of skeletal muscle mass using the D -Cr dilution method in prospective cohort studies may reveal sarcopenia as a powerful risk factor for late life disability and chronic disease.
肌肉减少症被描述为与年龄相关的骨骼肌质量下降。然而,几乎所有的肌肉减少症研究都测量了瘦体重(LBM)或去脂体重(FFM),而不是肌肉质量。在一些已发表的肌肉减少症研究中,LBM 或 FFM 被称为肌肉质量,导致人们错误地认为测量 LBM 或 FFM 是肌肉质量的准确衡量标准。因此,关于老年人 LBM 或 FFM 变化对功能能力、残疾和受伤性跌倒风险等结果的影响的数据不一致,导致得出肌肉质量与这些结果相关性较弱的结论。我们回顾并描述了最常用的身体成分测量方法的假设。双能 X 射线吸收法(DXA)已成为评估 LBM 或 FFM 和四肢瘦体重作为替代但不准确的肌肉质量测量的常用工具。其他以前使用的方法(全身水、生物电阻抗和成像)也有很大的局限性。D-肌酸(D-Cr)稀释法提供了肌酸池大小和骨骼肌质量的直接和准确测量。在最近一项针对老年男性(MrOS 队列)的研究中,D-Cr 肌肉质量与功能能力和受伤性跌倒及残疾风险相关,而 DXA 评估的 LBM 或四肢瘦体重与这些结果仅呈弱相关或不相关。DXA 和其他方法对肌肉质量的不准确测量导致结果不一致,并可能对骨骼肌质量在健康和疾病中的重要性得出错误结论。使用 D-Cr 稀释法在前瞻性队列研究中评估骨骼肌质量,可能会发现肌肉减少症是导致晚年残疾和慢性疾病的一个强有力的危险因素。