Lioufas Nicole, Hawley Carmel M, Cameron James D, Toussaint Nigel D
Department of Nephrology, The Royal Melbourne Hospital, Parkville, Australia.
Department of Medicine (RMH), University of Melbourne, Parkville, Australia.
Int J Hypertens. 2019 Feb 17;2019:9189362. doi: 10.1155/2019/9189362. eCollection 2019.
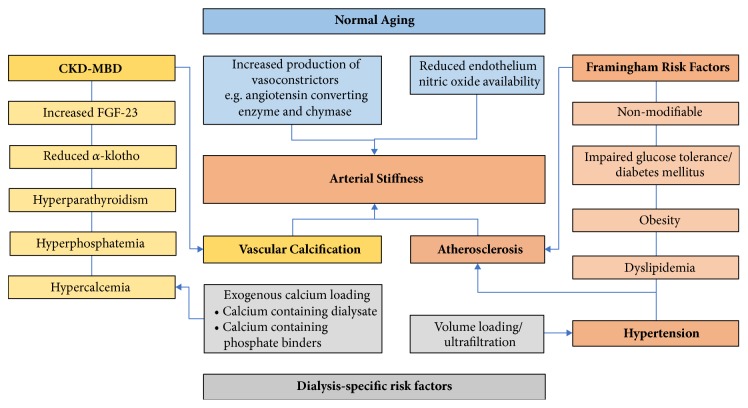
Chronic kidney disease (CKD) is associated with excess cardiovascular mortality, resulting from both traditional and nontraditional, CKD-specific, cardiovascular risk factors. Nontraditional risk factors include the entity Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD) which is characterised by disorders of bone and mineral metabolism, including biochemical abnormalities of hyperphosphatemia and hyperparathyroidism, renal osteodystrophy, and vascular calcification. Increased arterial stiffness in the CKD population can be attributed amongst other influences to progression of vascular calcification, with significant resultant contribution to the cardiovascular disease burden. Pulse wave velocity (PWV) measured over the carotid-femoral arterial segments is the noninvasive gold-standard technique for measurement of aortic stiffness and has been suggested as a surrogate cardiovascular end-point. A PWV value of 10 m/s or greater has been recommended as a suitable cut-off for an increased risk of cardiovascular mortality. CKD is a risk factor for an excessive rate of increase in aortic stiffness, reflected by increases in PWV, and increased aortic PWV in CKD shows faster progression than for individuals with normal kidney function. Patients with varying stages of CKD, as well as those on dialysis or with a kidney transplant, have different biological milieu which influence aortic stiffness and associated changes in PWV. This review discusses the pathophysiology of arterial stiffness with CKD and outlines the literature on PWV across the spectrum of CKD, highlighting that determination of arterial stiffness using aortic PWV can be a useful diagnostic and prognostic tool for assessing cardiovascular disease in the CKD population.
慢性肾脏病(CKD)与心血管疾病死亡率过高相关,这是由传统和非传统的、CKD特异性的心血管危险因素共同导致的。非传统危险因素包括慢性肾脏病-矿物质和骨代谢紊乱(CKD-MBD),其特征为骨和矿物质代谢紊乱,包括高磷血症和甲状旁腺功能亢进的生化异常、肾性骨营养不良以及血管钙化。CKD人群中动脉僵硬度增加在其他影响因素中可归因于血管钙化的进展,这对心血管疾病负担有显著的影响。测量颈股动脉段的脉搏波速度(PWV)是测量主动脉僵硬度的无创金标准技术,并已被建议作为替代心血管终点。建议将10米/秒或更高的PWV值作为心血管疾病死亡率增加风险的合适临界值。CKD是主动脉僵硬度过度增加速率的一个危险因素,表现为PWV升高,且CKD患者主动脉PWV升高的进展速度比肾功能正常者更快。不同阶段的CKD患者,以及接受透析或肾移植的患者,具有不同的生物环境,这些环境会影响主动脉僵硬度以及PWV的相关变化。本综述讨论了CKD时动脉僵硬度的病理生理学,并概述了CKD全病程中关于PWV的文献,强调使用主动脉PWV测定动脉僵硬度可作为评估CKD人群心血管疾病的有用诊断和预后工具。