Division of Vascular Surgery, Stanford University School of Medicine, Stanford, CA.
Center for Innovation to Implementation, VA Palo Alto Healthcare System, Palo Alto, CA.
Ann Surg. 2020 Dec;272(6):996-1005. doi: 10.1097/SLA.0000000000003276.
The Risk Analysis Index (RAI) predicts 30-, 180-, and 365-day mortality based on variables constitutive of frailty. Initially validated, in a single-center Veteran hospital, we sought to improve model performance by recalibrating the RAI in a large, veteran surgical registry, and to externally validate it in both a national surgical registry and a cohort of surgical patients for whom RAI was measured prospectively before surgery.
The RAI was recalibrated among development and confirmation samples within the Veterans Affairs Surgical Quality Improvement Program (VASQIP; 2010-2014; N = 480,731) including major, elective noncardiac surgery patients to create the revised RAI (RAI-rev), comparing discrimination and calibration. The model was tested externally in the American College of Surgeons National Surgical Quality Improvement Program dataset (NSQIP; 2005-2014; N = 1,391,785), and in a prospectively collected cohort from the Nebraska Western Iowa Health Care System VA (NWIHCS; N = 6,856).
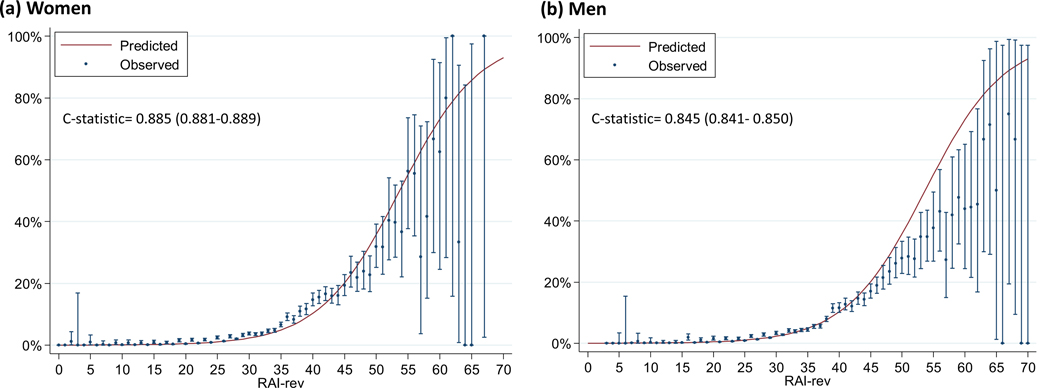
Recalibrating the RAI significantly improved discrimination for 30-day [c = 0.84-0.86], 180-day [c = 0.81-0.84], and 365-day mortality [c = 0.78-0.82] (P < 0.001 for all) in VASQIP. The RAI-rev also had markedly better calibration (median absolute difference between observed and predicted 180-day mortality: decreased from 8.45% to 1.23%). RAI-rev was highly predictive of 30-day mortality (c = 0.87) in external validation with excellent calibration (median absolute difference between observed and predicted 30-day mortality: 0.6%). The discrimination was highly robust in men (c = 0.85) and women (c = 0.89). Discrimination also improved in the prospectively measured cohort from NWIHCS for 180-day mortality [c = 0.77 to 0.80] (P < 0.001).
The RAI-rev has improved discrimination and calibration as a frailty-screening tool in surgical patients. It has robust external validity in men and women across a wide range of surgical settings and available for immediate implementation for risk assessment and counseling in preoperative patients.
风险分析指数(RAI)根据构成脆弱性的变量预测 30 天、180 天和 365 天的死亡率。最初在一家退伍军人单中心医院进行了验证,我们试图通过在退伍军人事务部手术质量改进计划(VASQIP;2010-2014 年)中的大型退伍军人手术登记处重新校准 RAI 来提高模型性能,并在全国手术登记处和前瞻性测量手术前 RAI 的手术患者队列中对其进行外部验证。
在 Veterans Affairs Surgical Quality Improvement Program(VASQIP;2010-2014 年)的开发和验证样本中重新校准 RAI,包括主要的、择期非心脏手术患者,以创建修订后的 RAI(RAI-rev),比较其区分度和校准度。该模型在 American College of Surgeons National Surgical Quality Improvement Program 数据集(NSQIP;2005-2014 年)中进行了外部测试,并在 Nebraska Western Iowa Health Care System VA(NWIHCS;6856 名)前瞻性收集的队列中进行了测试。
重新校准 RAI 显著提高了 VASQIP 中 30 天(c = 0.84-0.86)、180 天(c = 0.81-0.84)和 365 天死亡率(c = 0.78-0.82)的区分度(所有 P < 0.001)。RAI-rev 的校准也明显更好(观察到的 180 天死亡率和预测死亡率之间的中位数绝对差异:从 8.45%下降到 1.23%)。RAI-rev 在外部验证中对 30 天死亡率具有高度预测性(c = 0.87),且校准度极佳(观察到的 30 天死亡率和预测死亡率之间的中位数绝对差异:0.6%)。该区分度在男性(c = 0.85)和女性(c = 0.89)中均高度稳健。在 NWIHCS 的前瞻性测量队列中,180 天死亡率的区分度也有所提高[c = 0.77 至 0.80](P < 0.001)。
RAI-rev 作为一种用于手术患者的脆弱性筛查工具,其区分度和校准度得到了改善。它在广泛的手术环境中具有强大的外部有效性,适用于男性和女性,并且可立即用于术前患者的风险评估和咨询。