Infectious Diseases Institute, Makerere University College of Health Sciences, P.O. Box 22418, Kampala, Uganda.
Institute of Public Health, University of Cambridge, Cambridge, UK.
BMC Infect Dis. 2019 Mar 25;19(1):280. doi: 10.1186/s12879-019-3907-5.
The World Health Organisation approved boosted atazanavir as a preferred second line protease inhibitor in 2010. This is as an alternative to the current boosted lopinavir. Atazanavir has a lower genetic barrier than lopinavir. We compared the virological outcomes of patients during the roll out of routine viral load monitoring, who had switched to boosted second- line regimens of either atazanavir or lopinavir.
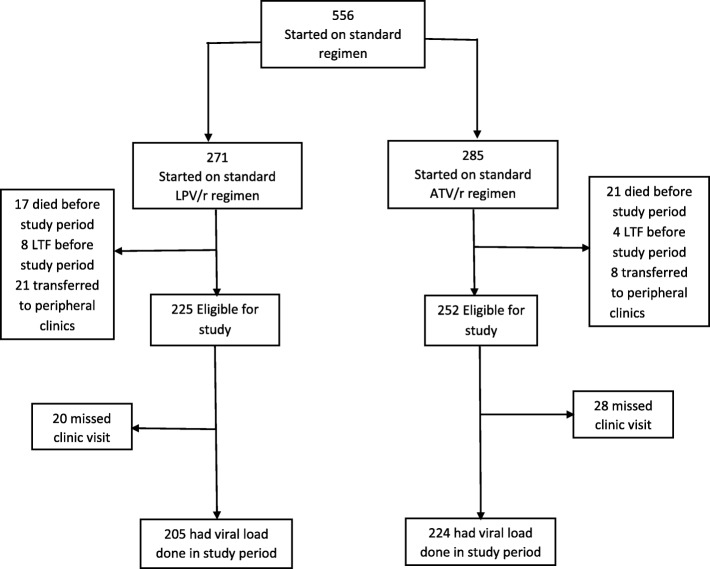
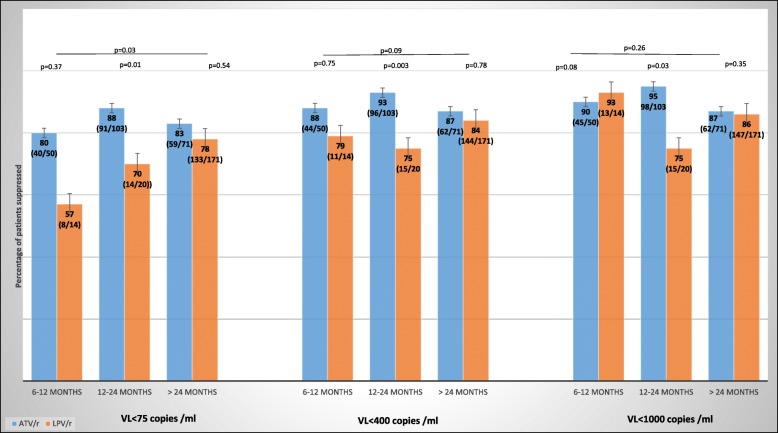
This was a cross-sectional study involving adult patients at the Infectious Diseases Institute Kampala, Uganda started on a standard WHO recommended second-line regimen containing either boosted atazanavir or boosted lopinavir between 1 Dec 2014 and 31 July 2015.. Mantel -Haenszel chi square was used to test for the statistical significance of the odds of being suppressed (VL < 400 copies/ml) when on boosted atazanavir compared to boosted lopinavir after stratifying by duration on antiretroviral therapy (ART). Multivariate logistic regression analysis used to determine if the type of boosted protease inhibitor (bPI) was associated with virological outcome.
Ninety (90) % on ATV/r and 83% on LPV/r had a VL less than 1000 copies/ml. The odds of being suppressed using the same viral load cut-off while on boosted atazanavir compared to boosted lopinavir was not statistically significant after stratifying for duration on ART (p = 0.09). In a multivariate analysis the type of bPI used was not a predictor of virological outcome (p = 0.60).
Patients using the WHO recommended second-line of boosted atazanavir have comparable virological suppression to those on boosted lopinavir.
世界卫生组织于 2010 年批准了强化阿扎那韦作为首选的二线蛋白酶抑制剂。这是替代当前强化洛匹那韦的方案。阿扎那韦的遗传屏障低于洛匹那韦。我们比较了在常规病毒载量监测推出期间,转换为强化二线方案的阿扎那韦或洛匹那韦的患者的病毒学结果。
这是一项横断面研究,涉及乌干达坎帕拉传染病研究所的成年患者,他们于 2014 年 12 月 1 日至 2015 年 7 月 31 日期间开始接受标准的世卫组织推荐的二线方案,方案中包含强化阿扎那韦或强化洛匹那韦。Mantel-Haenszel 卡方检验用于检验在强化阿扎那韦与强化洛匹那韦相比,在按抗逆转录病毒治疗(ART)时间分层后,病毒学抑制(VL<400 拷贝/ml)的几率是否具有统计学意义。多变量逻辑回归分析用于确定强化蛋白酶抑制剂(bPI)的类型是否与病毒学结果相关。
90%的 ATV/r 组和 83%的 LPV/r 组的病毒载量小于 1000 拷贝/ml。在按 ART 时间分层后,在强化阿扎那韦与强化洛匹那韦相比,使用相同的病毒载量截断值时,抑制的几率没有统计学意义(p=0.09)。在多变量分析中,使用的 bPI 类型不是病毒学结果的预测因素(p=0.60)。
使用世卫组织推荐的强化阿扎那韦二线方案的患者与强化洛匹那韦组相比,具有相似的病毒学抑制效果。