Division of Hematology, Oncology, and Bone Marrow Transplantation, University of Minnesota, Minneapolis, Minnesota.
Department of Internal Medicine, Mayo Clinic, Rochester, Minnesota.
Am J Hematol. 2019 Jun;94(6):658-666. doi: 10.1002/ajh.25473. Epub 2019 Apr 10.
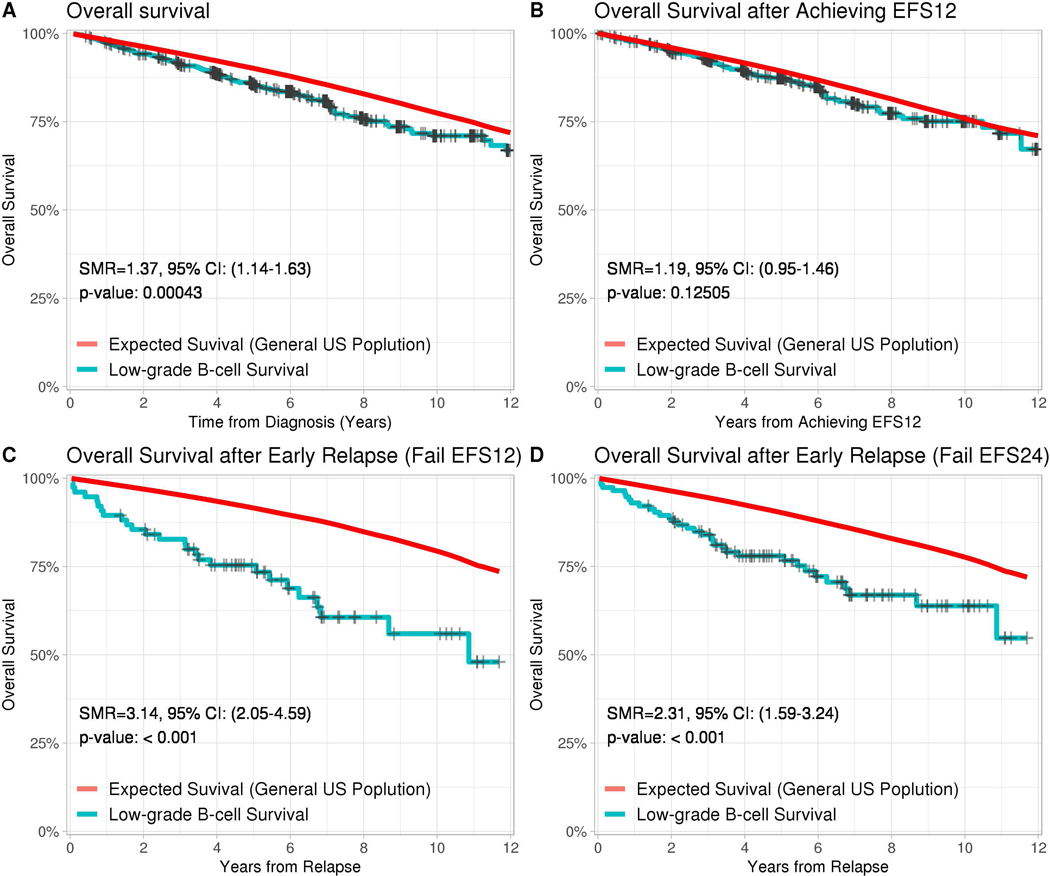
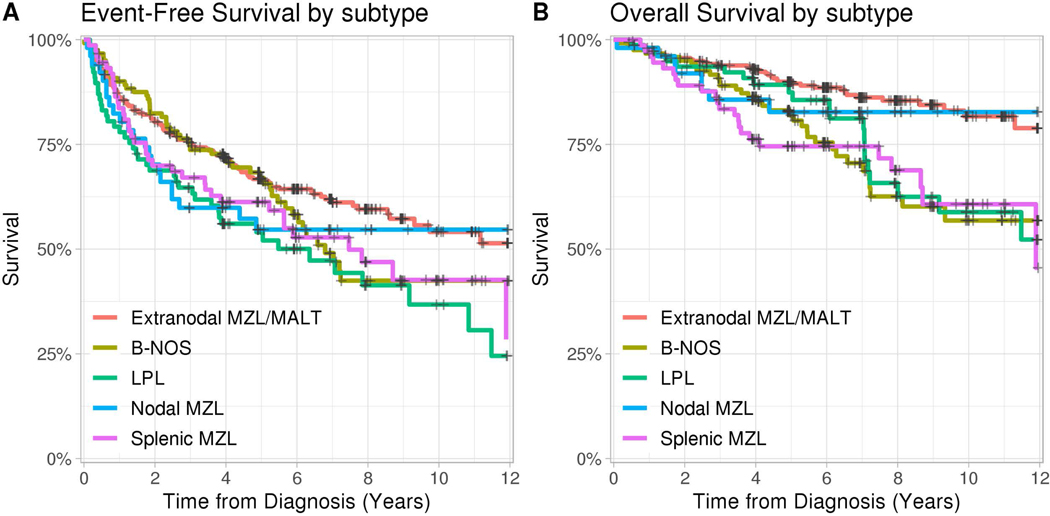
Indolent B-cell lymphomas other than follicular lymphoma account for up to 10% of all B-cell neoplasms. While they typically follow a slowly progressive course, some patients experience rapid progression and early mortality. Prognostic scoring systems have not been adopted, hindering the ability of clinicians or researchers to predict outcomes, or risk-stratify patients during clinical trials. To address this, we evaluated the utility of existing prognostic indices and novel, early disease-related outcomes, to predict subsequent long term survival. Baseline characteristics and outcomes data were generated from a longitudinal cohort study that prospectively enrolled 632 patients newly diagnosed with marginal zone lymphoma, lymphoplasmacytic lymphomas, or B-cell lymphomas not otherwise specified, beginning in 2002. The International Prognostic Index (IPI), Follicular Lymphoma International Prognostic Index (FLIPI), and MALT International prognostic index (MALT-IPI) demonstrated c-statistics that ranged from 0.593-0.612 for event-free survival (EFS), and 0.683-0.714 for overall survival (OS). Patients who attained event-free survival at 12 months (EFS12) experienced similar mortality to the US general population (standardized mortality ratio [SMR] 1.19; 95% CI 0.95-1.46). Patients who did not attain EFS12 had subsequent worse morality (SMR 3.14 (95% CI 2.05-4.59). The MALT-IPI demonstrated utility in predicting subsequent long-term outcomes among patients with non-follicular indolent B-cell lymphomas. This index should be used by clinicians giving guidance to patients at the time of initial diagnosis, and risk stratification during clinical studies. The divergent long-term outcomes experienced by patients who do or do not attain EFS12 suggest there exists a subset of patients who harbor high-risk disease. Future research efforts should focus on methods to identify these patients at the time of diagnosis, in order to enable risk-tailored therapy.
除滤泡性淋巴瘤以外的惰性 B 细胞淋巴瘤占所有 B 细胞肿瘤的 10%。虽然它们通常表现为缓慢进展的过程,但有些患者会出现快速进展和早期死亡。尚未采用预后评分系统,这阻碍了临床医生或研究人员预测结局或在临床试验中对患者进行风险分层的能力。为了解决这个问题,我们评估了现有的预后指标和新的早期疾病相关结局在预测后续长期生存方面的效用。基线特征和结局数据来自于一项纵向队列研究,该研究前瞻性地招募了 2002 年开始诊断为边缘区淋巴瘤、淋巴浆细胞淋巴瘤或未分类 B 细胞淋巴瘤的 632 例患者。国际预后指数(IPI)、滤泡性淋巴瘤国际预后指数(FLIPI)和黏膜相关淋巴组织淋巴瘤国际预后指数(MALT-IPI)在无事件生存(EFS)方面的 C 统计量范围为 0.593-0.612,在总生存(OS)方面的 C 统计量范围为 0.683-0.714。在 12 个月时达到无事件生存(EFS12)的患者与美国普通人群的死亡率相似(标准化死亡率比 [SMR] 1.19;95%CI 0.95-1.46)。未达到 EFS12 的患者随后的死亡率更高(SMR 3.14(95%CI 2.05-4.59)。MALT-IPI 在预测非滤泡性惰性 B 细胞淋巴瘤患者的后续长期结局方面具有一定的效用。该指数应在临床医生为初始诊断的患者提供指导时使用,并在临床研究中进行风险分层。达到或未达到 EFS12 的患者的长期结局不同,这表明存在一部分患者患有高危疾病。未来的研究工作应集中在诊断时识别这些患者的方法上,以便能够进行风险定制的治疗。