Emergency Department, The Affiliated Hospital of Zunyi Medical University, Zunyi, 563003, China.
The Affiliated Hospital of Zunyi Medical University, Zunyi, China.
Crit Care. 2019 Mar 27;23(1):100. doi: 10.1186/s13054-019-2389-6.
To evaluate the resuscitative effects of mechanical and manual chest compression in patients with out-of-hospital cardiac arrest (OHCA).
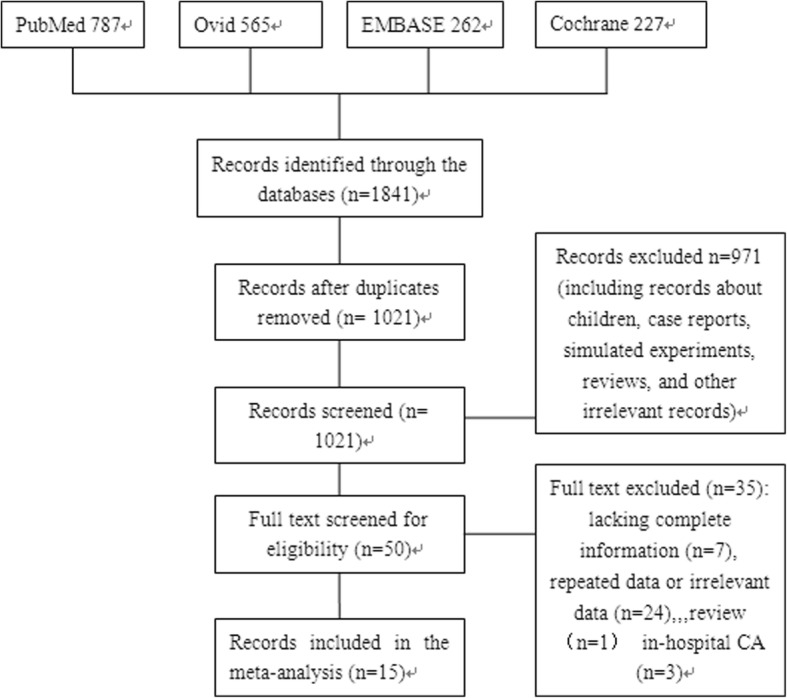
All randomized controlled and cohort studies comparing the effects of mechanical compression and manual compression on cardiopulmonary resuscitation in OHCA patients were retrieved from the Cochrane Library, PubMed, EMBASE, and Ovid databases from the date of their establishment to January 14, 2019. The included outcomes were as follows: the return of spontaneous circulation (ROSC) rate, the rate of survival to hospital admission, the rate of survival to hospital discharge, and neurological function. After evaluating the quality of the studies and summarizing the results, RevMan5.3 software was used for the meta-analysis.
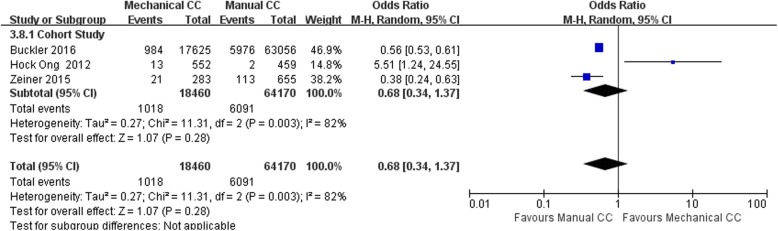
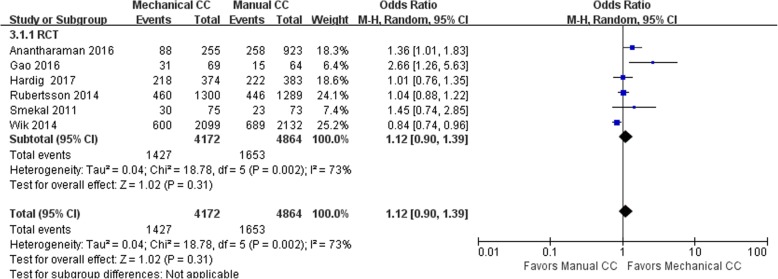
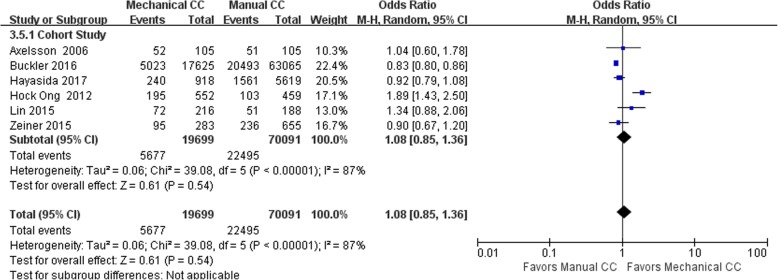
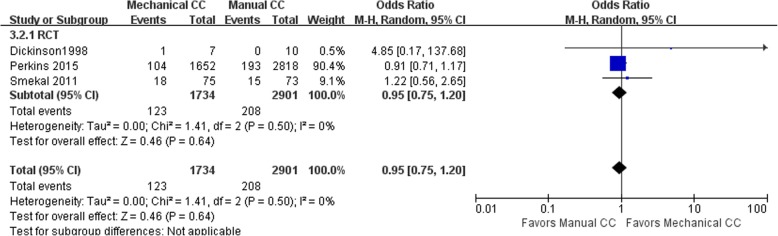
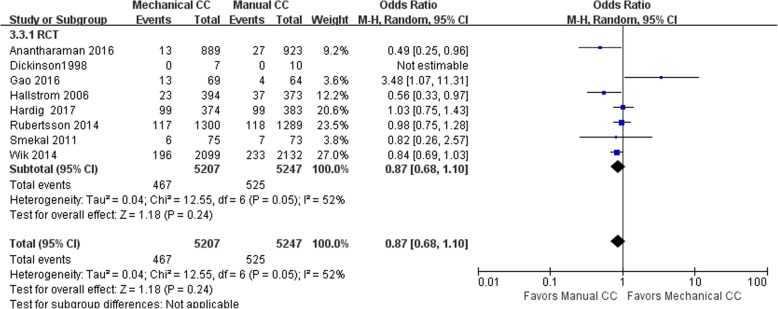
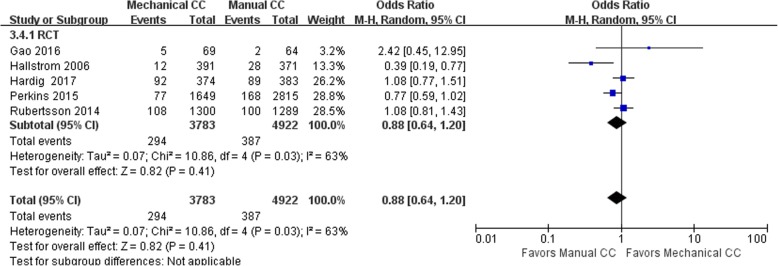
In total, 15 studies (9 randomized controlled trials and 6 cohort studies) were included. The results of the meta-analysis showed that there were no significant differences in the resuscitative effects of mechanical and manual chest compression in terms of the ROSC rate, the rate of survival to hospital admission and survival to hospital discharge, and neurological function in OHCA patients (ROSC: RCT: OR = 1.12, 95% CI (0.90, 1.39), P = 0.31; cohort study: OR = 1.08, 95% CI (0.85, 1.36), P = 0.54; survival to hospital admission: RCT: OR = 0.95, 95% CI (0.75, 1.20), P = 0.64; cohort study: OR = 0.98 95% CI (0.79, 1.20), P = 0.82; survival to hospital discharge: RCT: OR = 0.87, 95% CI (0.68, 1.10), P = 0.24; cohort study: OR = 0.78, 95% CI (0.53, 1.16), P = 0.22; Cerebral Performance Category (CPC) score: RCT: OR = 0.88, 95% CI (0.64, 1.20), P = 0.41; cohort study: OR = 0.68, 95% CI (0.34, 1.37), P = 0.28). When the mechanical compression group was divided into Lucas and Autopulse subgroups, the Lucas subgroup showed no difference from the manual compression group in ROSC, survival to admission, survival to discharge, and CPC scores; the Autopulse subgroup showed no difference from the manual compression subgroup in ROSC, survival to discharge, and CPC scores.
There were no significant differences in resuscitative effects between mechanical and manual chest compression in OHCA patients. To ensure the quality of CPR, we suggest that manual chest compression be applied in the early stage of CPR for OHCA patients, while mechanical compression can be used as part of advanced life support in the late stage.
评估机械和手动胸外按压在院外心脏骤停(OHCA)患者中的复苏效果。
从 Cochrane 图书馆、PubMed、EMBASE 和 Ovid 数据库中检索了自成立之日至 2019 年 1 月 14 日,比较机械按压和手动按压对 OHCA 患者心肺复苏效果的所有随机对照试验和队列研究。纳入的结局如下:自主循环恢复(ROSC)率、入院存活率、出院存活率和神经功能。评价研究质量并总结结果后,采用 RevMan5.3 软件进行荟萃分析。
共纳入 15 项研究(9 项随机对照试验和 6 项队列研究)。荟萃分析结果显示,机械和手动胸外按压在 OHCA 患者的 ROSC 率、入院存活率、出院存活率和神经功能方面的复苏效果无显著差异(ROSC:RCT:OR=1.12,95%CI(0.90,1.39),P=0.31;队列研究:OR=1.08,95%CI(0.85,1.36),P=0.54;入院存活率:RCT:OR=0.95,95%CI(0.75,1.20),P=0.64;队列研究:OR=0.98,95%CI(0.79,1.20),P=0.82;出院存活率:RCT:OR=0.87,95%CI(0.68,1.10),P=0.24;队列研究:OR=0.78,95%CI(0.53,1.16),P=0.22;Cerebral Performance Category(CPC)评分:RCT:OR=0.88,95%CI(0.64,1.20),P=0.41;队列研究:OR=0.68,95%CI(0.34,1.37),P=0.28)。当将机械按压组分为 Lucas 和 Autopulse 亚组时,Lucas 亚组在 ROSC、入院存活率、出院存活率和 CPC 评分方面与手动按压组无差异;Autopulse 亚组在 ROSC、出院存活率和 CPC 评分方面与手动按压亚组无差异。
在 OHCA 患者中,机械胸外按压和手动胸外按压在复苏效果方面无显著差异。为确保 CPR 质量,建议在 OHCA 患者 CPR 早期应用手动胸外按压,而机械按压可作为晚期高级生命支持的一部分。