Singapore Eye Research Institute, Singapore National Eye Centre, Singapore.
Ophthalmology and Visual Sciences Academic Clinical Program, Duke-NUS Medical School, Singapore.
JAMA Netw Open. 2019 Mar 1;2(3):e191540. doi: 10.1001/jamanetworkopen.2019.1540.
The association of diabetic microvascular complications such as diabetic retinopathy (DR) and diabetic kidney disease (DKD) with mortality in populations is not clear.
To examine the association of DR and DKD separately and jointly with all-cause and cardiovascular disease (CVD) mortality in a multiethnic Asian population.
DESIGN, SETTING, AND PARTICIPANTS: A population-based cohort study was conducted including 2964 adults between the ages of 40 and 80 years with diabetes who participated in the Singapore Epidemiology of Eye Diseases study (baseline, 2004-2011). Data analysis was performed from January to May 2018.
Diabetic retinopathy ascertained from retinal photographs and DKD from estimated glomerular filtration rate.
All-cause and CVD mortality obtained by linkage with the National Registry of Births and Deaths until May 2017.
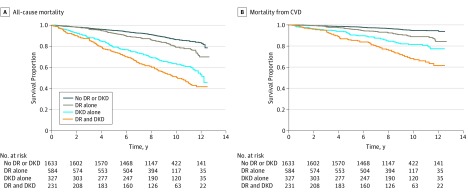
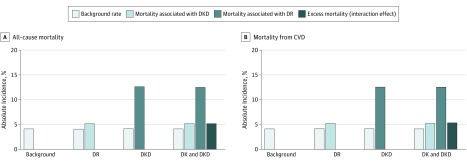
Of the 2964 adults (mean [SD] age, 61.8 [10.0] years; 1464 [49.4%] female; 592 Chinese, 1052 Malay, and 1320 Indian), 29.9% of the participants had DR, while 20.7% had DKD. Over a median (interquartile range) follow-up of 8.8 (7.2-11.0) years, 610 deaths occurred (20.6%), of which 267 (9.0%) were due to CVD. In separate models, the multivariable hazard ratios for all-cause and CVD mortality were 1.54 (95% CI, 1.24-1.91) and 1.74 (95% CI, 1.27-2.40), respectively, for DR and 2.04 (95% CI, 1.64-2.56) and 2.29 (95% CI, 1.64-3.19), respectively, for DKD. In models including both DR and DKD, the subgroup with DKD alone (27.1% and 12.6%) followed by DR alone (6.5% and 5.2%) contributed substantially to the excess risk of all-cause and CVD mortality. Compared with those with no DR and DKD, the hazard ratios of all-cause and CVD mortality were 1.89 (95% CI, 1.40-2.57) and 2.26 (95% CI, 1.42-3.61), respectively, for DKD alone and 1.38 (95% CI, 1.03-1.86) and 1.64 (95% CI, 1.06-2.56), respectively, for DR alone. Hazard ratios for all-cause and CVD mortality were 2.76 (95% CI, 2.05-3.72) and 3.41 (95% CI, 2.19-5.32), respectively, for those with both DKD and DR. The relative excess risk associated with the interaction was 0.49 (95% CI, -0.29 to 1.27; P = .20) for all-cause mortality and 0.51 (95% CI, -0.83 to 1.85; P = .50) for CVD mortality.
These results suggest that risks of all-cause and CVD mortality were significantly higher in those with DKD and DR, but DKD was more strongly associated with excess risk. The findings underscore the importance of early identification and close monitoring and management of patients with DR and DKD to reduce the risk of death.
糖尿病微血管并发症(如糖尿病视网膜病变[DR]和糖尿病肾病[DKD])与死亡率之间的关系在人群中尚不清楚。
在一个多民族亚洲人群中,分别检查 DR 和 DKD 与全因和心血管疾病(CVD)死亡率的关联。
设计、地点和参与者:进行了一项基于人群的队列研究,包括 2964 名年龄在 40 至 80 岁之间患有糖尿病的成年人,他们参加了新加坡眼病流行病学研究(基线,2004-2011 年)。数据分析于 2018 年 1 月至 5 月进行。
通过视网膜照片确定糖尿病视网膜病变,通过估计肾小球滤过率确定糖尿病肾病。
通过与国家出生和死亡登记处的链接获得全因和 CVD 死亡率,直到 2017 年 5 月。
在 2964 名成年人中(平均[SD]年龄,61.8[10.0]岁;1464[49.4%]女性;592 名中国人、1052 名马来人、1320 名印度人),29.9%的参与者患有 DR,而 20.7%的参与者患有 DKD。在中位数(四分位距)8.8(7.2-11.0)年的随访中,发生了 610 例死亡(20.6%),其中 267 例(9.0%)死于 CVD。在单独的模型中,全因和 CVD 死亡率的多变量危险比分别为 1.54(95%CI,1.24-1.91)和 1.74(95%CI,1.27-2.40),DR 为 2.04(95%CI,1.64-2.56)和 2.29(95%CI,1.64-3.19),DR 为 2.04(95%CI,1.64-2.56)和 2.29(95%CI,1.64-3.19)。在包括 DR 和 DKD 的模型中,仅 DKD (27.1%和 12.6%)随后是仅 DR (6.5%和 5.2%)的亚组对全因和 CVD 死亡率的超额风险贡献很大。与无 DR 和 DKD 的患者相比,仅 DKD 的全因和 CVD 死亡率的危险比分别为 1.89(95%CI,1.40-2.57)和 2.26(95%CI,1.42-3.61),仅 DR 的全因和 CVD 死亡率的危险比分别为 1.38(95%CI,1.03-1.86)和 1.64(95%CI,1.06-2.56)。全因和 CVD 死亡率的危险比分别为 2.76(95%CI,2.05-3.72)和 3.41(95%CI,2.19-5.32),对于同时患有 DKD 和 DR 的患者。与交互作用相关的相对超额风险为 0.49(95%CI,-0.29 至 1.27;P=0.20)用于全因死亡率,0.51(95%CI,-0.83 至 1.85;P=0.50)用于 CVD 死亡率。
这些结果表明,患有 DKD 和 DR 的患者全因和 CVD 死亡率的风险明显更高,但 DKD 与超额风险的相关性更强。这些发现强调了早期识别和密切监测和管理 DR 和 DKD 患者以降低死亡风险的重要性。