AP-HM Hôpital de la Timone, Service de Pharmacologie Clinique et Pharmacovigilance, 264 rue Saint Pierre, 13005, Marseille, France.
AP-HP Hôpital Cochin, Service de Pharmacologie, 27 rue du Faubourg St-Jacques, 75679, Paris Cedex 14, France.
Crit Care. 2019 Mar 29;23(1):104. doi: 10.1186/s13054-019-2378-9.
Beta-lactam antibiotics (βLA) are the most commonly used antibiotics in the intensive care unit (ICU). ICU patients present many pathophysiological features that cause pharmacokinetic (PK) and pharmacodynamic (PD) specificities, leading to the risk of underdosage. The French Society of Pharmacology and Therapeutics (SFPT) and the French Society of Anaesthesia and Intensive Care Medicine (SFAR) have joined forces to provide guidelines on the optimization of beta-lactam treatment in ICU patients.
A consensus committee of 18 experts from the two societies had the mission of producing these guidelines. The entire process was conducted independently of any industry funding. A list of questions formulated according to the PICO model (Population, Intervention, Comparison, and Outcomes) was drawn-up by the experts. Then, two bibliographic experts analysed the literature published since January 2000 using predefined keywords according to PRISMA recommendations. The quality of the data identified from the literature was assessed using the GRADE® methodology. Due to the lack of powerful studies having used mortality as main judgement criteria, it was decided, before drafting the recommendations, to formulate only "optional" recommendations.
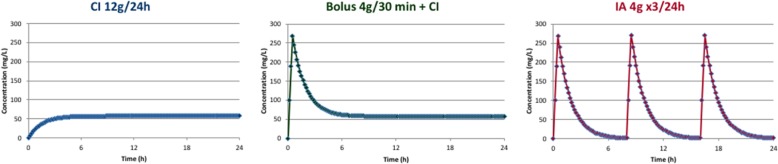
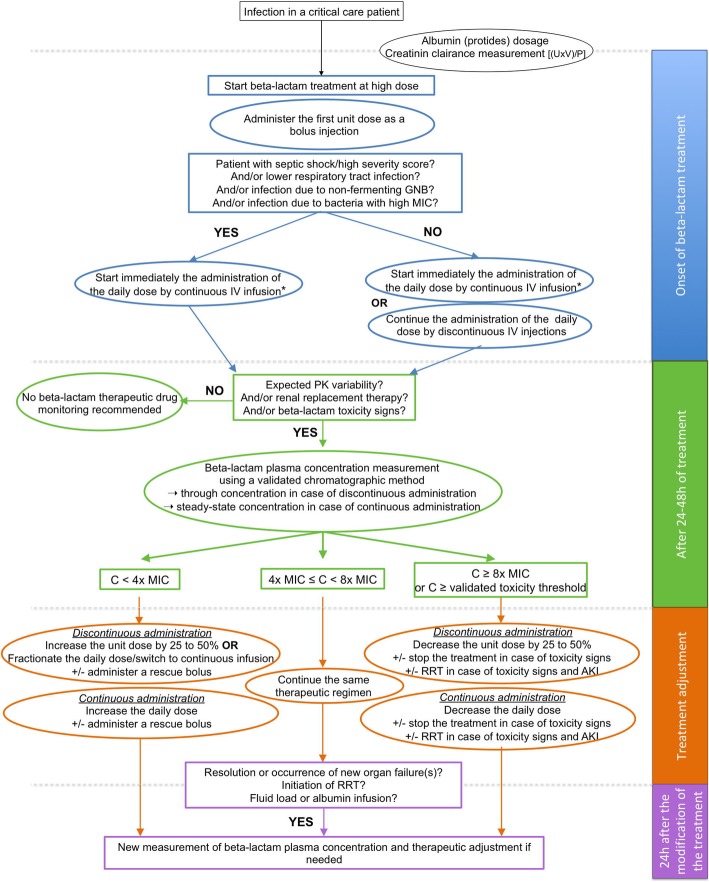
After two rounds of rating and one amendment, a strong agreement was reached by the SFPT-SFAR guideline panel for 21 optional recommendations and a recapitulative algorithm for care covering four areas: (i) pharmacokinetic variability, (ii) PK-PD relationship, (iii) administration modalities, and (iv) therapeutic drug monitoring (TDM). The most important recommendations regarding βLA administration in ICU patients concerned (i) the consideration of the many sources of PK variability in this population; (ii) the definition of free plasma concentration between four and eight times the Minimal Inhibitory Concentration (MIC) of the causative bacteria for 100% of the dosing interval as PK-PD target to maximize bacteriological and clinical responses; (iii) the use of continuous or prolonged administration of βLA in the most severe patients, in case of high MIC bacteria and in case of lower respiratory tract infection to improve clinical cure; and (iv) the use of TDM to improve PK-PD target achievement.
The experts strongly suggest the use of personalized dosing, continuous or prolonged infusion and therapeutic drug monitoring when administering βLA in critically ill patients.
β-内酰胺类抗生素(βLA)是重症监护病房(ICU)中最常用的抗生素。ICU 患者表现出许多导致药代动力学(PK)和药效学(PD)特异性的病理生理学特征,导致剂量不足的风险。法国药理学和治疗学学会(SFPT)和法国麻醉与重症监护医学学会(SFAR)已联手为 ICU 患者β-内酰胺治疗的优化提供指南。
由来自两个学会的 18 名专家组成的共识委员会承担了制定这些指南的任务。整个过程独立于任何行业资助进行。专家们根据 PICO 模型(人群、干预、比较和结局)制定了一份问题清单。然后,两名文献专家根据 PRISMA 建议使用预定义的关键字分析了自 2000 年 1 月以来发表的文献。使用 GRADE®方法评估从文献中确定的数据质量。由于缺乏使用死亡率作为主要判断标准的有力研究,因此在起草建议之前,决定仅制定“可选”建议。
经过两轮评分和一次修订,SFPT-SFAR 指南小组就 21 项可选建议和涵盖四个方面的护理总结算法达成强烈共识:(i)药代动力学变异性,(ii)PK-PD 关系,(iii)给药方式,和(iv)治疗药物监测(TDM)。关于 ICU 患者βLA 给药的最重要建议涉及(i)考虑该人群中许多 PK 变异性的来源;(ii)将游离血浆浓度定义为引起细菌的最小抑菌浓度(MIC)的 4 到 8 倍,作为 PK-PD 目标,以最大限度地提高细菌学和临床反应;(iii)在最严重的患者、高 MIC 细菌和下呼吸道感染的情况下,使用连续或延长βLA 给药,以提高临床治愈率;和(iv)使用 TDM 提高 PK-PD 目标的实现。
专家强烈建议在危重症患者中使用个体化给药、连续或延长输注和治疗药物监测βLA。