Department of Internal Medicine I, University of Bonn, Bonn, Germany.
Department of Clinical Medicine, Sapienza University of Rome, Rome, Italy.
Clin Transl Gastroenterol. 2019 Apr;10(4):e00025. doi: 10.14309/ctg.0000000000000025.
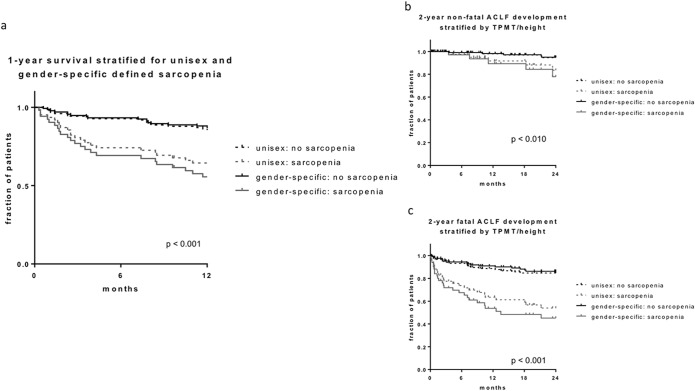
Muscle mass has been shown to be a prognostic marker in patients with liver cirrhosis. Transversal psoas muscle thickness normalized by height (TPMT/height) obtained by routine computed tomography is a simple surrogate parameter for sarcopenia. TPMT/height, however, is not sex specific, which might play a role in risk stratification. Its association with acute-on-chronic liver failure (ACLF) has not been established yet. ACLF is associated with systemic inflammatory dysregulation. This study aimed at evaluating the role of sarcopenia in ACLF development of patients with decompensated cirrhosis receiving transjugular intrahepatic portosystemic shunt (TIPS) using sex-specific TPMT/height.
One hundred eighty-six patients from the prospective Non-invasive Evaluation Program for TIPS and Follow Up Network cohort (observational, real-world TIPS cohort with structured follow-up) were analyzed. TPMT/height was measured from routine computed tomography. The sex-specific cutoff was determined to classify patients as sarcopenic and nonsarcopenic for 1-year mortality after TIPS. Clinical outcome was compared. Primary end points were ACLF and 1-year mortality after TIPS. Secondary end points were development of decompensations (hepatic encephalopathy and ascites) after TIPS.
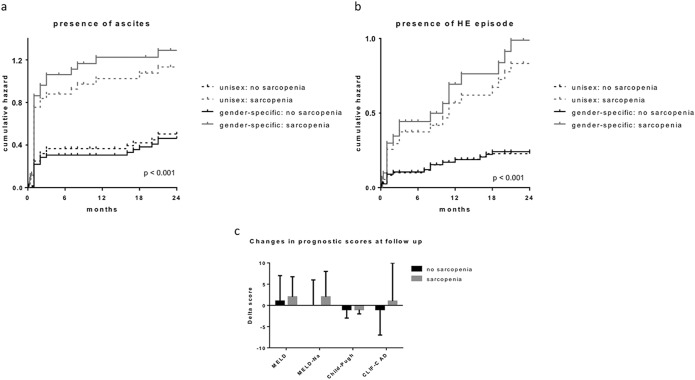
The sex-specific cutoff increases the diagnostic accuracy with regard to primary and secondary end points compared with the unisex cutoff. Sex-specific sarcopenia classification is an independent predictor of 1-year mortality and ACLF development in patients with cirrhosis receiving TIPS. Patients in the sarcopenia group showed significantly higher rates of mortality, ascites, overt hepatic encephalopathy, and ACLF after TIPS compared with the nonsarcopenia group. The Chronic Liver Failure Consortium Acute Decompensation score as a marker of systemic inflammation was significantly higher in sarcopenic patients.
This study demonstrates for the first time that sarcopenia is related to ACLF development and systemic inflammation. The prognostic value of TPMT/height can be improved by using sex-specific cutoffs. ClinicalTrials.gov identifier: NCT03584204.
肌肉质量已被证明是肝硬化患者的预后标志物。通过常规计算机断层扫描获得的经身高标准化的横突旁肌厚度(TPMT/身高)是肌少症的简单替代参数。然而,TPMT/身高不是性别特异性的,这可能在风险分层中起作用。其与慢加急性肝衰竭(ACLF)的关系尚未确定。ACLF 与全身炎症失调有关。本研究旨在评估使用性别特异性 TPMT/身高评估接受经颈静脉肝内门体分流术(TIPS)的失代偿性肝硬化患者 ACLF 发展中的肌少症的作用。
分析了前瞻性非侵入性 TIPS 评估和随访网络队列(观察性、具有结构化随访的真实世界 TIPS 队列)中的 186 名患者。从常规计算机断层扫描中测量 TPMT/身高。确定性别特异性截止值以将患者分类为肌少症和非肌少症,以预测 TIPS 后 1 年的死亡率。比较临床结果。主要终点是 TIPS 后 ACLF 和 1 年死亡率。次要终点是 TIPS 后出现失代偿(肝性脑病和腹水)。
与通用截止值相比,性别特异性截止值增加了主要和次要终点的诊断准确性。性别特异性肌少症分类是接受 TIPS 的肝硬化患者 1 年死亡率和 ACLF 发展的独立预测因子。与非肌少症组相比,肌少症组患者在 TIPS 后死亡率、腹水、显性肝性脑病和 ACLF 的发生率明显更高。作为全身炎症标志物的慢性肝脏衰竭联盟急性失代偿评分在肌少症患者中明显更高。
本研究首次证明肌少症与 ACLF 发展和全身炎症有关。使用性别特异性截止值可以提高 TPMT/身高的预后价值。临床试验标识符:NCT03584204。