Department of Gastroenterology, Hepatology and Nutrition, The University of Texas MD Anderson Cancer Center, Unit 1466, 1515 Holcombe Blvd, Houston, TX, 77030, USA.
Department of Biostatistics, The University of Texas MD Anderson Cancer Center, Houston, TX, USA.
J Immunother Cancer. 2019 Apr 2;7(1):93. doi: 10.1186/s40425-019-0577-1.
Current treatment guidelines for immune-mediated colitis (IMC) recommend 4 to 6 weeks of steroids as first-line therapy, followed by selective immunosuppressive therapy (SIT) (infliximab or vedolizumab) in patients who do not respond to steroids. We assessed the effect of early SIT introduction and number of SIT infusions on clinical outcomes.
We performed a retrospective review of patients with IMC who received SIT at The University of Texas MD Anderson Cancer Center between January and December 2018. Logistic regression analyses were used to assess associations between clinical outcomes and features of IMC.
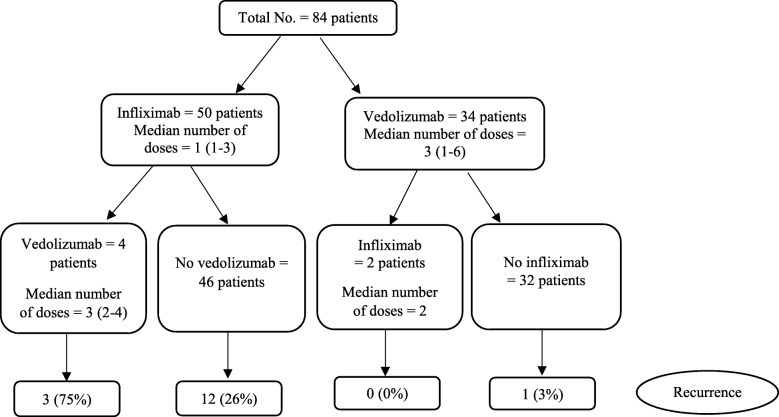
Of the 1459 patients who received immune checkpoint inhibitors, 179 developed IMC of any grade; 84 of these 179 patients received SIT. Of the 84 patients who received SIT, 79% were males, and the mean age was 60 years (standard deviation, 14). Compared with patients who received SIT > 10 days after IMC onset, patients who received early SIT (≤10 days) required fewer hospitalizations (P = 0.03), experienced steroid taper failure less frequently (P = 0.03), had fewer steroid tapering attempts (P < 0.01), had a shorter course of steroid treatment (P = 0.09), and had a shorter duration of symptoms (P < 0.01). Patients who received one or two infusions of SIT achieved histologic remission less frequently (P = 0.09) and had higher fecal calprotectin levels after SIT (P = 0.01) compared with patients who received three or more infusions. Risk factors for IMC recurrence after weaning off steroids included: 1) needing multiple hospitalizations, 2) experiencing steroid taper failure after SIT, 3) receiving infliximab rather than vedolizumab, 4) receiving fewer than three infusions of SIT, 5) having higher fecal calprotectin levels after SIT, and 6) receiving a longer course of steroids, hospitalization and IMC symptoms. Unsuccessful weaning from steroids after SIT was associated with high IMC grades; multiple hospitalizations; steroid-resistant IMC; long interval from IMC to SIT initiation; and long duration of steroids, IMC symptoms, and hospitalization.
SIT should be introduced early in the disease course of IMC instead of waiting until failure of steroid therapy or steroid taper. Patients who received three or more infusions of SIT had more favorable clinical outcomes.
目前,免疫介导性结肠炎(IMC)的治疗指南建议,对于类固醇治疗无应答的患者,在使用 4 至 6 周的类固醇后,应采用选择性免疫抑制治疗(SIT)(英夫利昔单抗或维得利珠单抗)。我们评估了 SIT 早期引入和 SIT 输注次数对临床结局的影响。
我们对 2018 年 1 月至 12 月期间在德克萨斯大学 MD 安德森癌症中心接受 SIT 的 IMC 患者进行了回顾性研究。采用逻辑回归分析评估了 IMC 特征与临床结局之间的关联。
在接受免疫检查点抑制剂治疗的 1459 例患者中,有 179 例发生任何等级的 IMC;其中 84 例患者接受了 SIT。在接受 SIT 的 84 例患者中,79%为男性,平均年龄为 60 岁(标准差为 14)。与 IMC 发病后接受 SIT 治疗>10 天的患者相比,早期(≤10 天)接受 SIT 治疗的患者住院次数更少(P=0.03),类固醇减量失败的频率更低(P=0.03),类固醇减量尝试次数更少(P<0.01),类固醇治疗时间更短(P=0.09),症状持续时间更短(P<0.01)。接受 1 或 2 次 SIT 输注的患者达到组织学缓解的频率较低(P=0.09),且 SIT 后粪便钙卫蛋白水平较高(P=0.01)。类固醇停药后 IMC 复发的风险因素包括:1)需要多次住院治疗;2)SIT 后类固醇减量失败;3)接受英夫利昔单抗而非维得利珠单抗治疗;4)接受少于 3 次 SIT 治疗;5)SIT 后粪便钙卫蛋白水平较高;6)接受较长时间的类固醇、住院和 IMC 症状治疗。SIT 后类固醇治疗不能成功减停与 IMC 严重程度较高、多次住院、类固醇难治性 IMC、从 IMC 到 SIT 开始的时间间隔较长、以及类固醇、IMC 症状和住院时间较长有关。
在 IMC 病程早期而不是在类固醇治疗失败或类固醇减量时应尽早引入 SIT。接受 3 次或更多次 SIT 输注的患者具有更有利的临床结局。