Botswana Harvard AIDS Institute Partnership, Gaborone, Botswana.
Department of Immunology and Infectious Diseases, Harvard T.H. Chan School of Public Health, Boston, USA.
AIDS. 2019 May 1;33(6):1073-1082. doi: 10.1097/QAD.0000000000002166.
Scale-up of antiretroviral therapy (ART) and introduction of treat-all strategy necessitates population-level monitoring of acquired HIV drug resistance (ADR) and pretreatment drug resistance (PDR) mutations.
Blood samples were collected from 4973 HIV-positive individuals residing in 30 communities across Botswana who participated in the Botswana Combination Prevention Project (BCPP) in 2013-2018. HIV sequences were obtained by long-range HIV genotyping. Major drug-resistance mutations (DRMs) and surveillance drug resistance mutations (SDRMs) associated with nucleoside reverse transcriptase inhibitors (NRTI) and nonnucleoside reverse transcriptase inhibitors (NNRTI) were analyzed according to the Stanford University HIV Drug Resistance Database. Viral sequences were screened for G-to-A hypermutations. A threshold of 2% was used for hypermutation adjustment. Viral suppression was considered at HIV-1 RNA load ≤400 copies/ml.
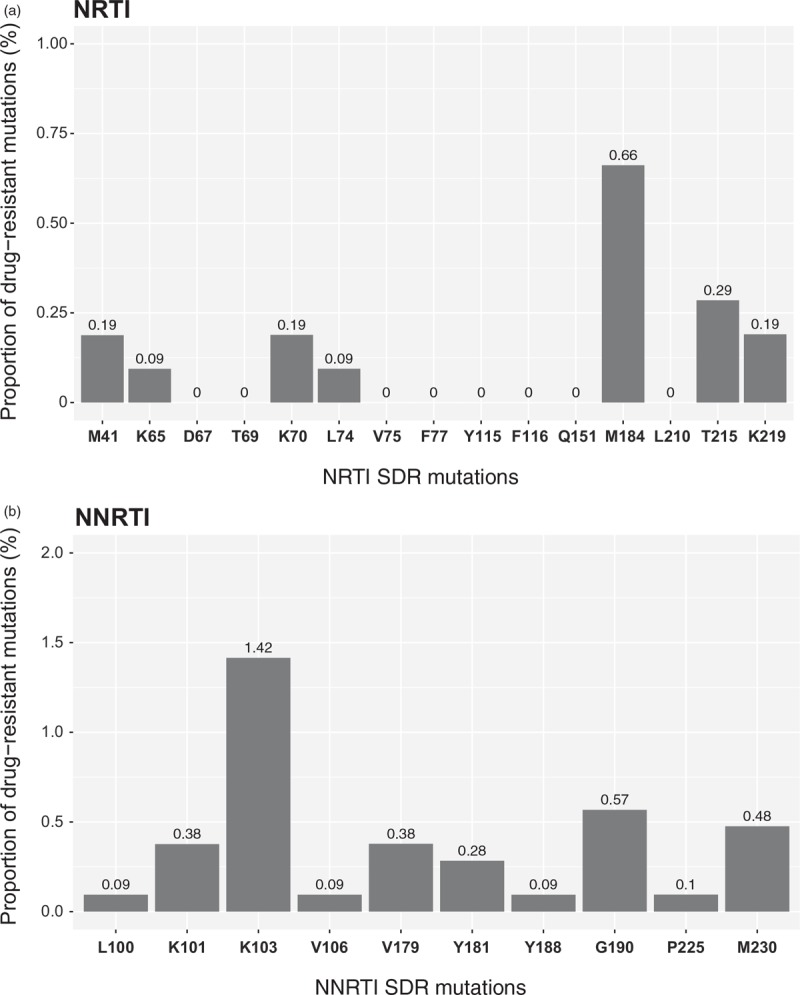
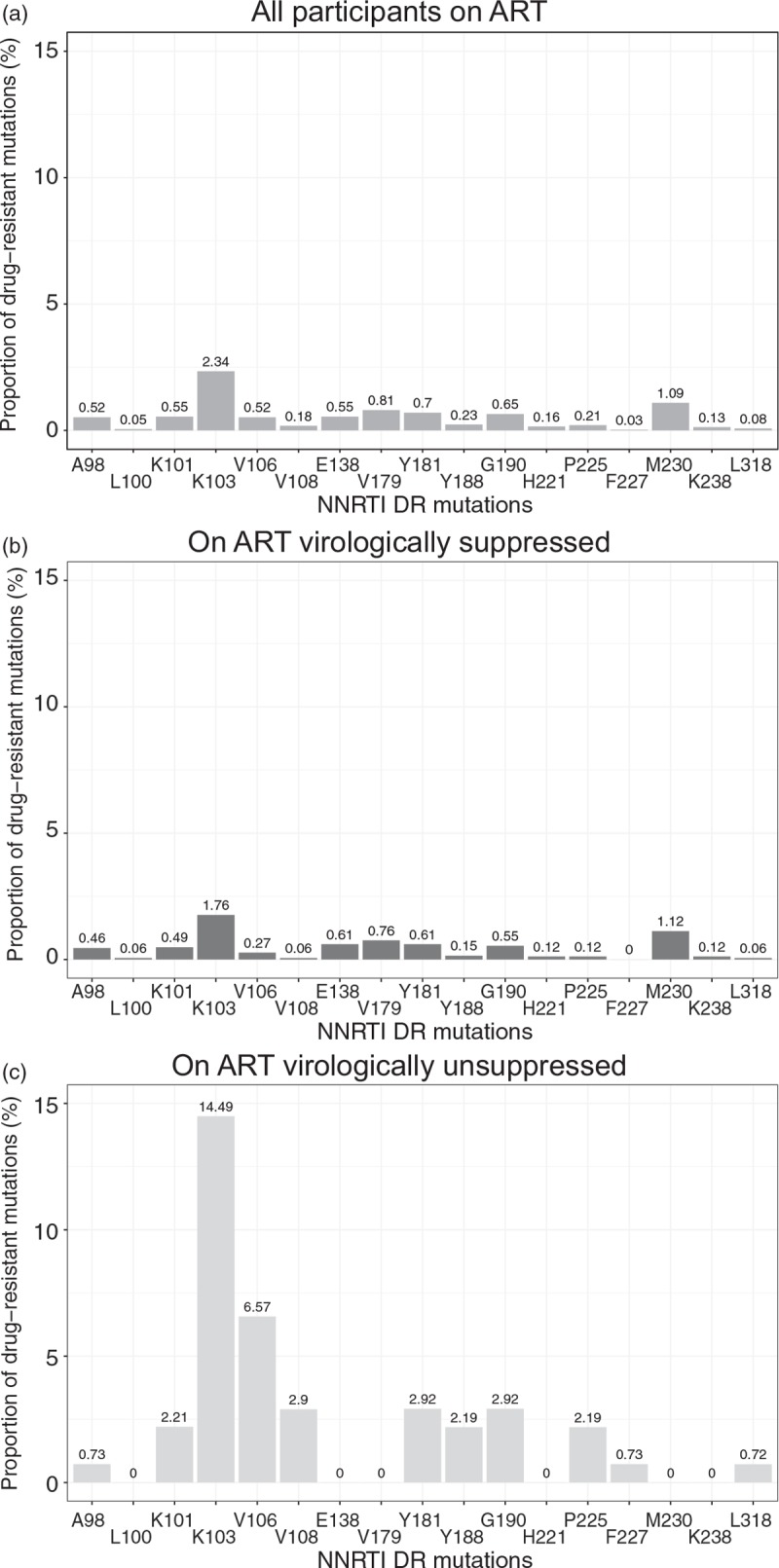
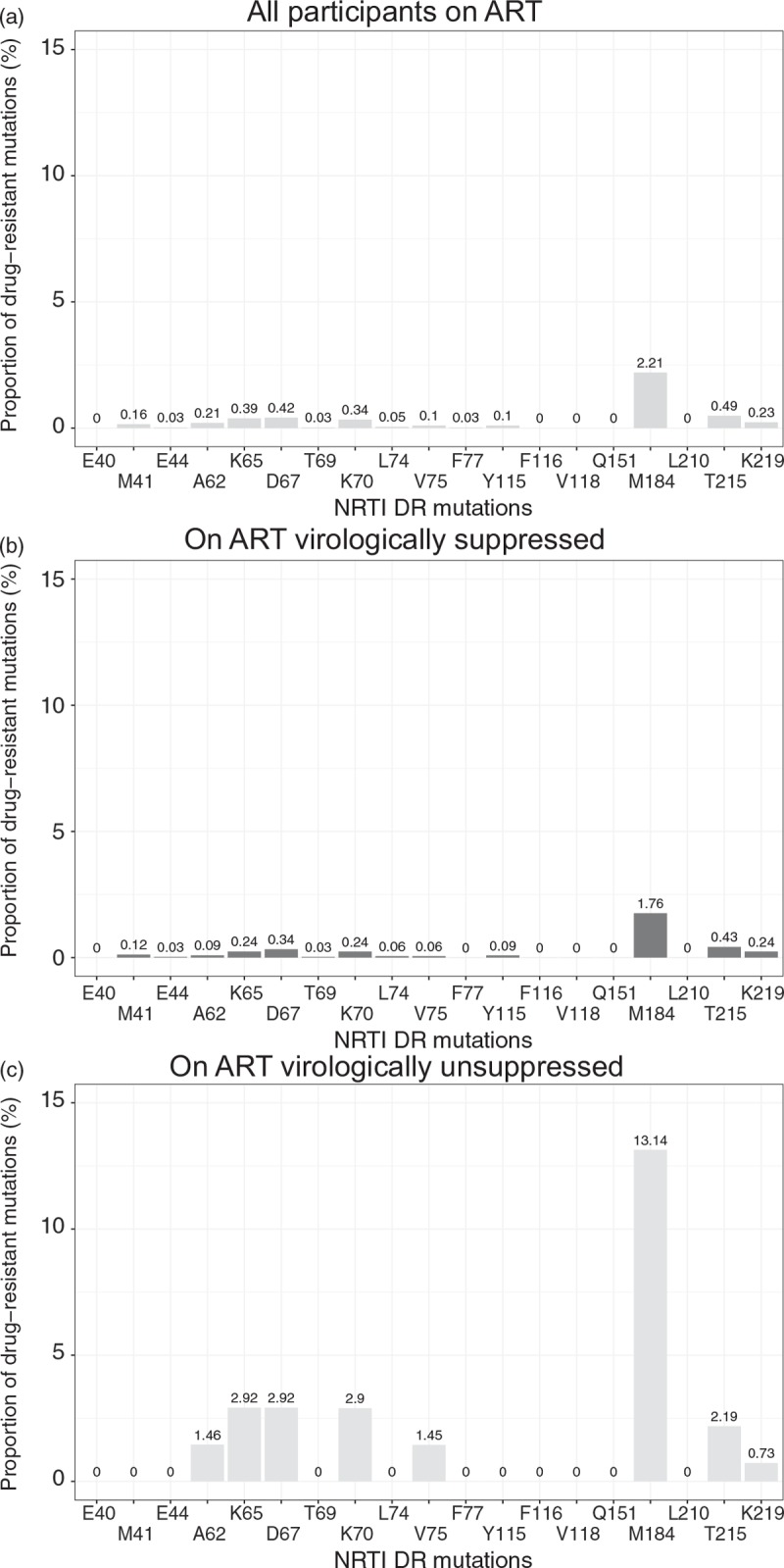
Among 4973 participants with HIV-1C sequences, ART data were available for 4927 (99%) including 3858 (78%) on ART. Among those on ART, 3435 had viral load data and 3297 (96%) were virologically suppressed. Among 1069 (22%) HIV-infected individuals not on ART, we found NRTI-associated and NNRTI-associated SDRMs were found in 1.5% (95% confidence interval [CI] 1.0-2.5%) and 2.9% (95% CI 2.0-4.2%), respectively. Of the 138 (4%) of individuals who had detectable HIV-1 RNA, we found NRTI-associated and NNRTI-associated drug resistance mutations in 16% (95% CI 10-25%) and 33% (95% CI 25-42%), respectively.
We found a low prevalence of NRTI-associated and NNRTI-associated PDR-resistance mutations among residents of rural and peri-urban communities across Botswana. However, individuals on ART with detectable virus had ADR NRTI and NNRTI mutations above 15%.
抗逆转录病毒疗法(ART)的推广和治疗所有策略的引入需要在人群水平上监测获得性 HIV 耐药(ADR)和治疗前耐药(PDR)突变。
从居住在博茨瓦纳 30 个社区的 4973 名 HIV 阳性个体中采集血液样本,这些个体参加了 2013 年至 2018 年的博茨瓦纳联合预防项目(BCPP)。通过长距离 HIV 基因分型获得 HIV 序列。根据斯坦福大学 HIV 耐药数据库,分析与核苷逆转录酶抑制剂(NRTI)和非核苷逆转录酶抑制剂(NNRTI)相关的主要耐药突变(DRMs)和监测耐药突变(SDRMs)。对病毒序列进行 G 到 A 超突变筛查。使用 2%的阈值进行超突变调整。当 HIV-1 RNA 载量≤400 拷贝/ml 时,认为病毒得到抑制。
在 4973 名携带 HIV-1C 序列的参与者中,有 4927 名(99%)提供了 ART 数据,其中 3858 名(78%)正在接受 ART。在接受 ART 的人群中,3435 人有病毒载量数据,其中 3297 人(96%)病毒得到抑制。在未接受 ART 的 1069 名(22%)HIV 感染者中,我们发现 NRTI 相关和 NNRTI 相关的 SDRMs 分别为 1.5%(95%置信区间[CI] 1.0-2.5%)和 2.9%(95% CI 2.0-4.2%)。在 138 名(4%)可检测到 HIV-1 RNA 的个体中,我们发现 NRTI 相关和 NNRTI 相关的耐药突变分别为 16%(95% CI 10-25%)和 33%(95% CI 25-42%)。
我们发现博茨瓦纳农村和城乡结合社区居民中 NRTI 相关和 NNRTI 相关 PDR 耐药突变的流行率较低。然而,接受 ART 治疗且病毒可检测的个体中,ADR NRTI 和 NNRTI 突变率高于 15%。