Bareng Ontlametse T, Choga Wonderful T, Maphorisa Segomotso T, Seselamarumo Sekgabo, Seatla Kaelo K, Mokgethi Patrick T, Maruapula Dorcas, Mogwele Mompati L, Ditshwanelo Doreen, Moraka Natasha O, Gobe Irene, Motswaledi Modisa S, Makhema Joseph M, Musonda Rosemary, Shapiro Roger, Essex Max, Novitsky Vlad, Moyo Sikhulile, Gaseitsiwe Simani
Botswana Harvard AIDS Institute Partnership, Gaborone, Botswana.
School of Allied Health Professions, Faculty of Health Sciences, University of Botswana, Gaborone, Botswana.
Infect Drug Resist. 2022 Dec 22;15:7565-7576. doi: 10.2147/IDR.S388816. eCollection 2022.
Monitoring HIV-1 drug resistance mutations (DRM) in treated patients on combination antiretroviral therapy (cART) with a detectable HIV-1 viral load (VL) is important for the selection of appropriate cART. Currently, there is limited data on HIV DRM at low-level viremia (LLV) (VL 401-999 copies/mL) due to the use of a threshold of VL ≥1000 copies/mL for HIV DRM testing. We here assess the performance of an in-house HIV drug resistance genotyping assay using plasma for the detection of DRM at LLV.
We used a total of 96 HIV plasma samples from the population-based Botswana Combination Prevention Project (BCPP). The samples were stratified by VL groups: 50 samples had LLV, defined as 401-999 copies/mL, and 46 had ≥1000 copies/mL. HIV pol (PR and RT) region was amplified and sequenced using an in-house genotyping assay with BigDye sequencing chemistry. Known HIV DRMs were identified using the Stanford HIV Drug Resistance Database. Genotyping success rate between the two groups was estimated and compared using the comparison of proportions test.
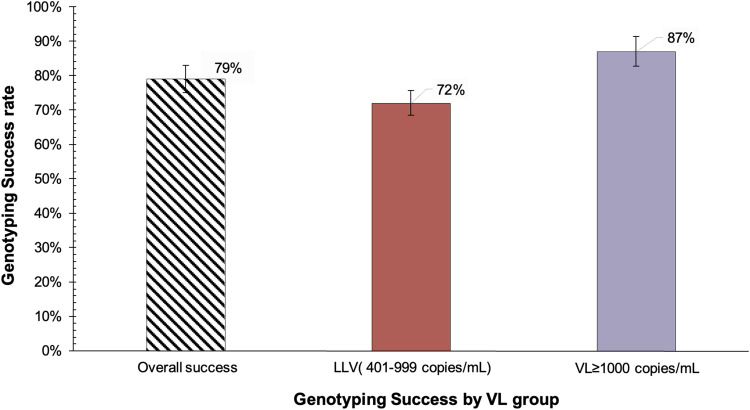
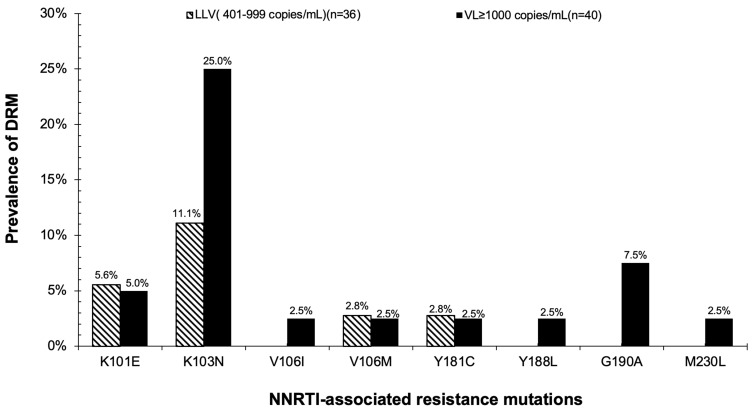
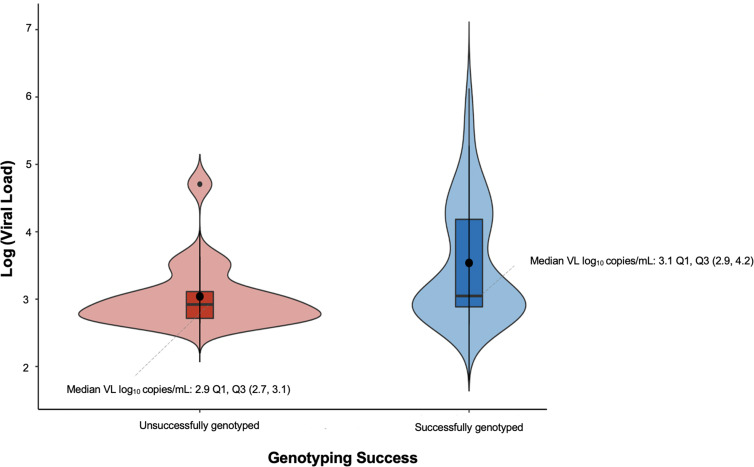
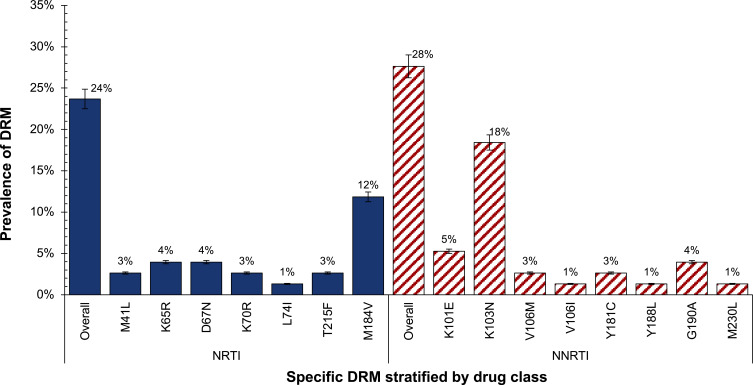
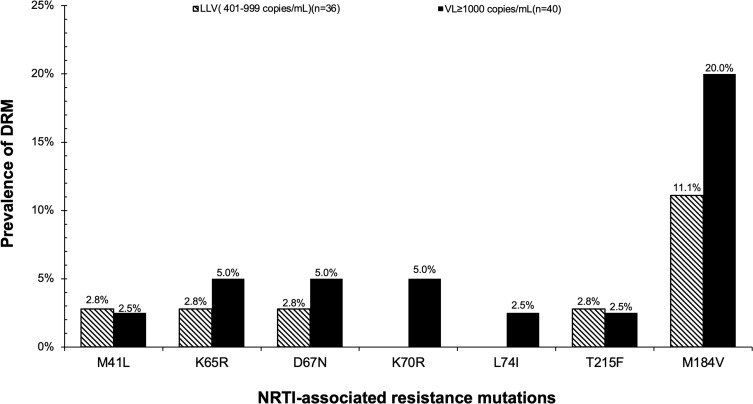
The overall genotyping success rate was 79% (76/96). For VL groups, the genotyping success was 72% (36/50) at LLV and 87% (40/46) at VL ≥1000 copies/mL. Among generated sequences, the overall prevalence of individuals with at least 1 major or intermediate-associated DRM was 24% (18/76). The proportions of NNRTI-, NRTI- and PI-associated resistance mutations were 28%, 24%, and 0%, respectively. The most predominant mutations detected were K103N (18%) and M184V (12%) in NNRTI- and NRTI-associated mutations, respectively. The prevalence of DRM was 17% (6/36) at LLV and 30% (12/40) at VL ≥1000 copies/mL.
The in-house HIV genotyping assay successfully genotyped 72% of LLV samples and was able to detect 17% of DRM amongst them. Our results highlight the possibility and clinical significance of genotyping HIV among individuals with LLV.
监测接受联合抗逆转录病毒疗法(cART)且可检测到HIV-1病毒载量(VL)的患者中的HIV-1耐药性突变(DRM),对于选择合适的cART至关重要。目前,由于HIV DRM检测使用的VL阈值为≥1000拷贝/毫升,关于低水平病毒血症(LLV,VL为401 - 999拷贝/毫升)时HIV DRM的数据有限。我们在此评估一种使用血浆检测LLV时DRM的内部HIV耐药基因分型检测方法的性能。
我们总共使用了来自基于人群的博茨瓦纳联合预防项目(BCPP)的96份HIV血浆样本。样本按VL组分层:50份样本为LLV,定义为401 - 999拷贝/毫升,46份样本的VL≥1000拷贝/毫升。使用带有BigDye测序化学的内部基因分型检测方法对HIV pol(蛋白酶和逆转录酶)区域进行扩增和测序。使用斯坦福HIV耐药数据库鉴定已知的HIV DRM。使用比例比较检验估计并比较两组之间的基因分型成功率。
总体基因分型成功率为79%(76/96)。对于VL组,LLV时基因分型成功率为72%(36/50),VL≥1000拷贝/毫升时为87%(40/46)。在生成的序列中,至少有1个主要或中度相关DRM的个体总体患病率为24%(18/76)。与非核苷类逆转录酶抑制剂(NNRTI)、核苷类逆转录酶抑制剂(NRTI)和蛋白酶抑制剂(PI)相关的耐药性突变比例分别为28%、24%和0%。检测到的最主要突变分别是NNRTI相关突变中的K103N(18%)和NRTI相关突变中的M184V(12%)。LLV时DRM患病率为17%(6/36),VL≥1000拷贝/毫升时为30%(12/40)。
内部HIV基因分型检测方法成功地对72%的LLV样本进行了基因分型,并能够在其中检测到17%的DRM。我们的结果突出了对LLV个体进行HIV基因分型的可能性和临床意义。