1 Saint Luke's Mid America Heart Institute/University of Missouri Kansas City Kansas City MO.
2 Cardiovascular Research Foundation New York NY.
J Am Heart Assoc. 2019 Apr 16;8(8):e011529. doi: 10.1161/JAHA.118.011529.
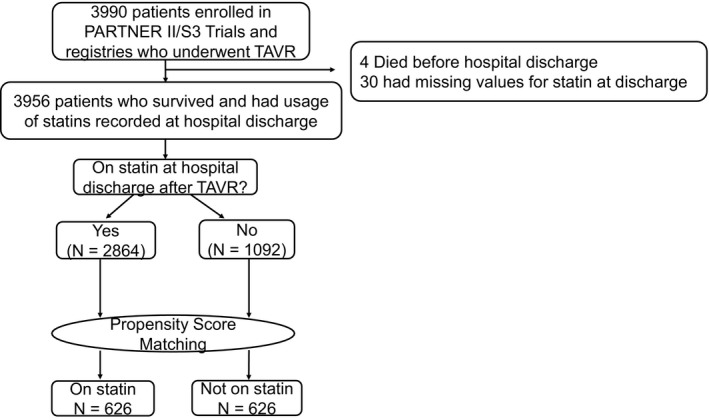
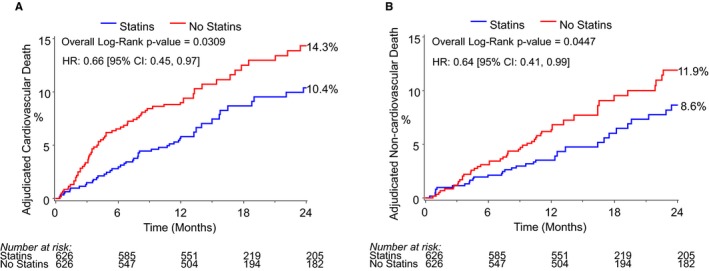
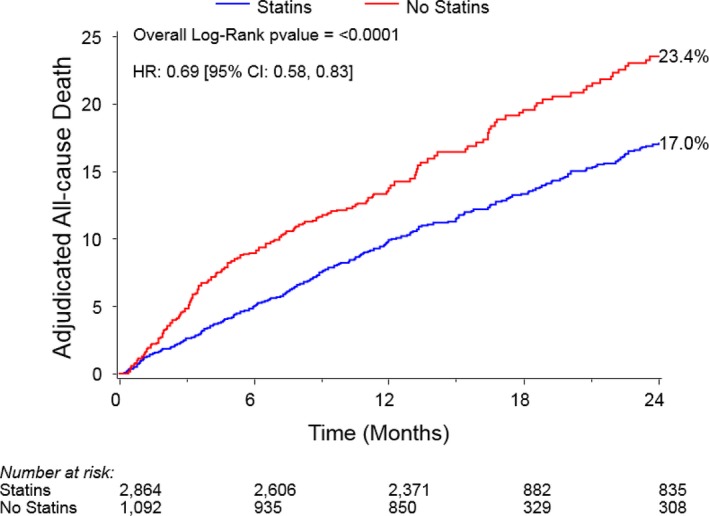
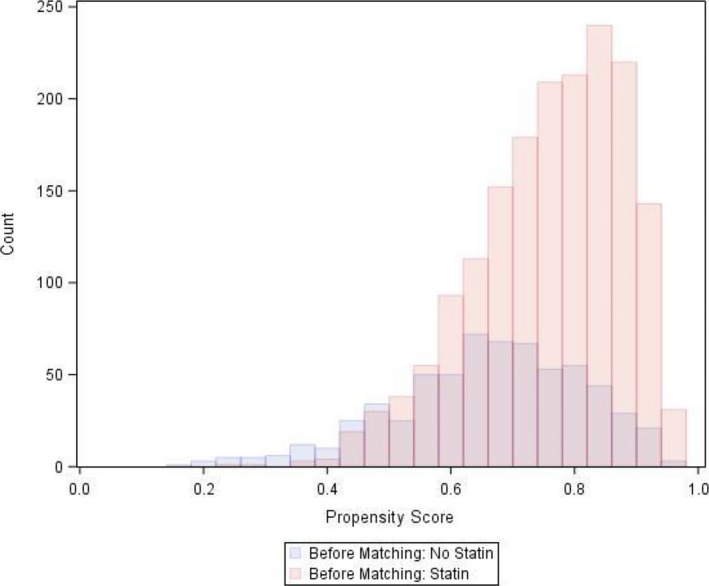
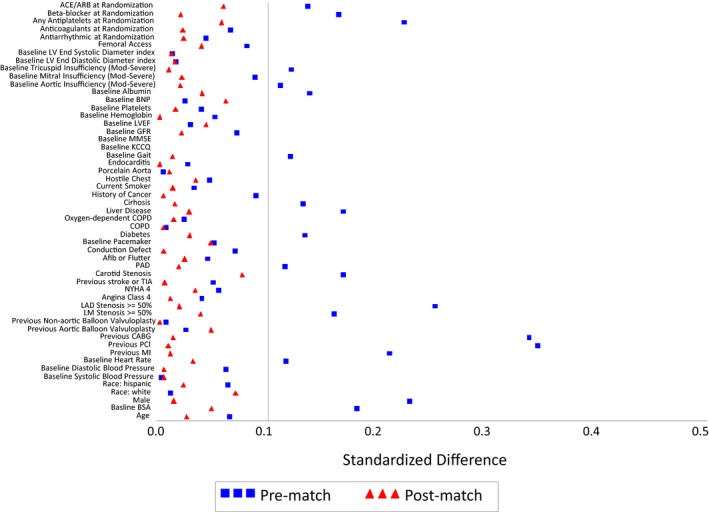
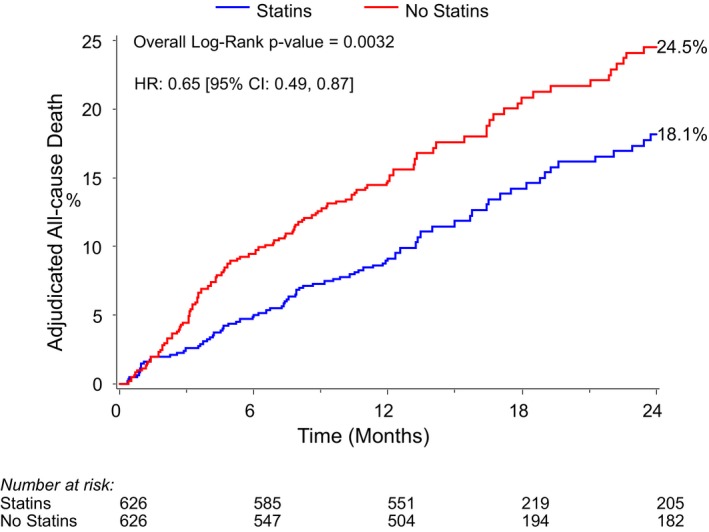
Background Statins may reduce mortality after transcatheter aortic valve replacement (TAVR) through prevention of atherosclerotic events or pleiotropic effects. However, the competing mortality risks in TAVR patients may dilute any positive effect of statins. We sought to understand the association of statin use with post-TAVR mortality. Methods and Results We included high- or intermediate-surgical risk patients who underwent TAVR as a part of the PARTNER (Placement of Aortic Transcatheter Valves) II and Sapien 3 trials and registries. Outcomes included 2-year all-cause, cardiovascular, and noncardiovascular mortality. We used propensity score matching to generate matched pairs between those discharged on a statin and those not on a statin after TAVR. Bias was explored with falsification end points (urinary infection, hip fracture). Among 3956 patients who underwent TAVR, we matched 626 patients on a statin with 626 patients not on a statin at discharge. Among matched patients, statin use was associated with lower risk of all-cause (hazard ratio [HR] 0.65, 95% CI 0.49-0.87, P=0.001), cardiovascular (HR 0.66, 95% CI 0.46-0.96, P=0.030), and noncardiovascular mortality (HR 0.64, 95% CI 0.44-0.99, P=0.045) compared with no statin use. The survival curves diverged within 3 months and continued to separate over a median follow-up of 2.1 years. The falsification end points were similar among groups (urinary infection, P=0.66; hip fracture, P=0.64). Conclusions In an observational, propensity-matched analysis of TAVR patients, statin use was associated with lower rates of cardiovascular and noncardiovascular mortality compared with no statin use. Given the early emergence of the apparent protective effect of statins, this result may be driven either by pleiotropic effects or by residual confounding despite propensity-matching methodology.
他汀类药物通过预防动脉粥样硬化事件或多效作用可能降低经导管主动脉瓣置换术(TAVR)后的死亡率。然而,TAVR 患者的竞争死亡风险可能会稀释他汀类药物的任何积极作用。我们试图了解他汀类药物使用与 TAVR 后死亡率之间的关系。
我们纳入了 PARTNER(主动脉经导管瓣膜置换术)II 和 Sapien 3 试验和注册研究中接受 TAVR 的高或中手术风险患者。结局包括 2 年全因、心血管和非心血管死亡率。我们使用倾向评分匹配在 TAVR 后出院时使用他汀类药物和未使用他汀类药物的患者之间生成匹配对。使用伪造终点(尿路感染、髋部骨折)探索偏倚。在 3956 例接受 TAVR 的患者中,我们匹配了 626 例出院时使用他汀类药物的患者和 626 例未使用他汀类药物的患者。在匹配患者中,与未使用他汀类药物相比,使用他汀类药物与全因死亡风险降低相关(风险比 [HR]0.65,95%CI0.49-0.87,P=0.001)、心血管死亡风险(HR0.66,95%CI0.46-0.96,P=0.030)和非心血管死亡率(HR0.64,95%CI0.44-0.99,P=0.045)。生存曲线在 3 个月内出现分歧,并在中位随访 2.1 年后继续分离。各组的伪造终点相似(尿路感染,P=0.66;髋部骨折,P=0.64)。
在 TAVR 患者的观察性、倾向评分匹配分析中,与未使用他汀类药物相比,使用他汀类药物与较低的心血管和非心血管死亡率相关。鉴于他汀类药物的这种明显保护作用的早期出现,尽管采用了倾向评分匹配方法,但该结果可能是由多效作用或残留混杂因素驱动的。