Department of Radiation Oncology, Medical University of South Carolina, Charleston.
Department of Cell and Molecular Pharmacology, Medical University of South Carolina, Charleston.
JAMA Netw Open. 2019 Apr 5;2(4):e191703. doi: 10.1001/jamanetworkopen.2019.1703.
Previous studies have shown that continued smoking among patients with cancer can increase overall and cancer-specific mortality, risk for second primary cancer, and risk for toxic effects of cancer treatment. To our knowledge, there have been no efforts to estimate additional costs for cancer treatment attributed to smoking.
To model attributable incremental costs of subsequent cancer treatment associated with continued smoking by patients with cancer.
DESIGN, SETTING, AND PARTICIPANTS: For this economic evaluation, a model was developed in 2018 using data from a 2014 US Surgeon General's report that considered expected failure rates of first-line cancer treatment in nonsmoking patients, smoking prevalence, odds ratio of first-line cancer treatment failure attributed to smoking compared with nonsmoking, and cost of cancer treatment after failure of first-line cancer treatment.
Attributable failures of first-line cancer treatment and incremental cost for subsequent treatment associated with continued smoking among patients with cancer.
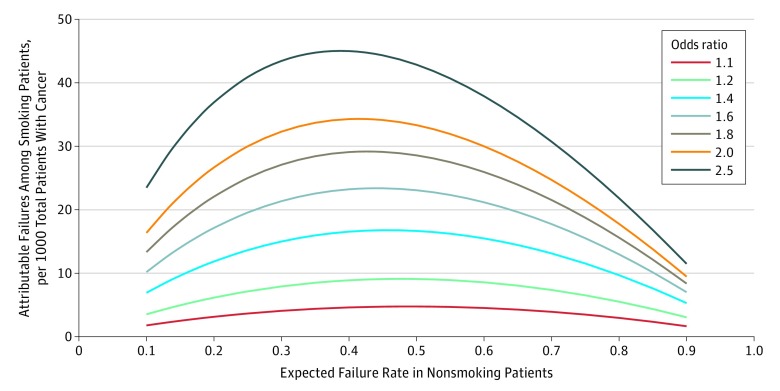
Attributable treatment failures were higher under conditions in which high first-line cure rates were expected in nonsmoking patients compared with conditions in which low cure rates were expected. Peak attributable failures occurred under the conditions in which expected cure rates among nonsmoking patients ranged from 50% to 65%. Under the conditions of a 30% expected treatment failure rate among nonsmoking patients, 20% smoking prevalence, 60% increased risk of failure of first-line cancer treatment, and $100 000 mean added cost of treating a first-line cancer treatment failure, the additional incremental cost per 1000 total patients was estimated to be $2.1 million, reflecting an additional cost of $10 678 per smoking patient. Extrapolation of cost to 1.6 million patients with cancer diagnosed annually reflects a potential $3.4 billion in incremental cost.
The findings suggest that continued smoking among patients with cancer and the increase in attributable first-line cancer treatment failure is associated with significant incremental costs for subsequent cancer treatments. Additional work appears to be needed to identify optimal methods to mitigate these incremental costs.
先前的研究表明,癌症患者持续吸烟会增加总体和癌症特异性死亡率、第二原发癌风险以及癌症治疗毒性作用的风险。据我们所知,尚未有研究估算吸烟导致癌症治疗增量成本。
评估癌症患者持续吸烟导致后续癌症治疗的增量成本。
设计、地点和参与者:在这项经济评估中,我们于 2018 年使用源自 2014 年美国卫生局局长报告的数据开发了一个模型,该报告考虑了非吸烟患者一线癌症治疗的预期失败率、吸烟流行率、归因于吸烟的一线癌症治疗失败的比值比、以及一线癌症治疗失败后的癌症治疗成本。
归因于一线癌症治疗失败和与癌症患者持续吸烟相关的后续治疗的增量成本。
在非吸烟患者预期高一线治愈率的情况下,归因于治疗失败的治疗失败率更高,而非吸烟患者预期低治愈率的情况下则更低。在非吸烟患者预期治愈率在 50%至 65%之间的情况下,归因于治疗失败的发生率达到峰值。在非吸烟患者 30%的预期治疗失败率、20%的吸烟流行率、60%的一线癌症治疗失败风险增加和 100000 美元治疗一线癌症治疗失败的平均增量成本的情况下,估计每 1000 名患者的额外增量成本为 210 万美元,反映出每名吸烟患者的额外成本为 10678 美元。将成本外推至每年诊断的 160 万名癌症患者,潜在增量成本为 34 亿美元。
研究结果表明,癌症患者持续吸烟以及归因于一线癌症治疗失败的增加与后续癌症治疗的显著增量成本相关。似乎需要开展更多工作来确定减轻这些增量成本的最佳方法。