Kidney Transplant Program, St. Michael's Hospital, University of Toronto, 61 Queen Street East, 9th Floor, Toronto, ON, M5C 2T2, Canada.
Department of Medicine, University of Toronto, Toronto, ON, Canada.
BMC Infect Dis. 2019 Apr 5;19(1):311. doi: 10.1186/s12879-019-3944-0.
Trimethoprim-sulfamethoxazole (TMP-SMX) is the drug of choice for anti-Pneumocystis jirovecii pneumonia (PcP) prophylaxis in kidney transplant recipients (KTR). Post-transplant management balances preventing PcP with managing TMP-SMX-related adverse effects. TMP-SMX dose reduction addresses adverse effects but its implications to incident PcP are unclear.
We performed a retrospective review of all patients transplanted between 2011 and 2015 prescribed daily single strength TMP-SMX for twelve months post-transplantation as PcP prophylaxis. Actual TMP-SMX dose and duration, adverse effects, number of dose reductions and reasons, and PcP events were captured. Multivariate logistic regression analyses for risk factors associated with dose reduction were performed.
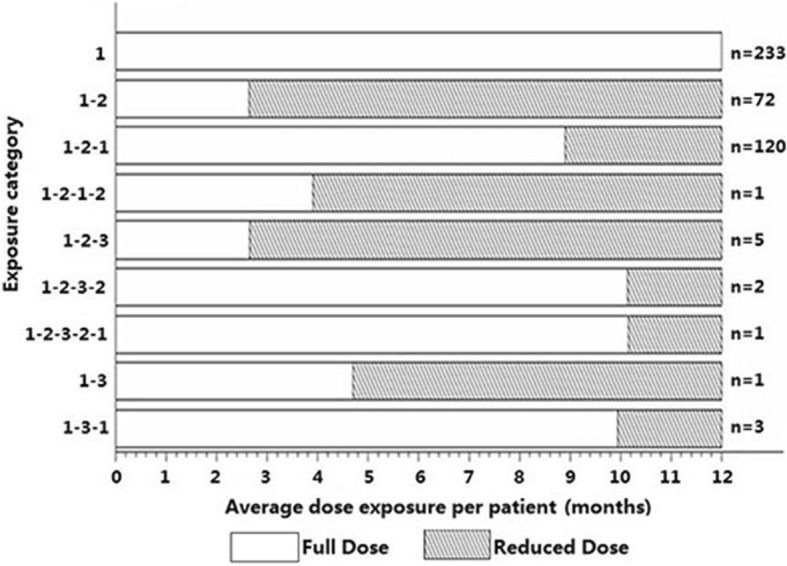
Of 438 KTR, 233 (53%) maintained daily TMP-SMX and 205 (47%) sustained ≥1 dose reduction, with the point prevalence of a reduced dose regimen being between 18 and 25%. Median duration for daily TMP-SMX was 8.45/12 months, contributing 4137 patient-months daily TMP-SMX and 1110 patient-months with a reduced dose. PcP did not occur in any patients. There were 84 documented dose reductions for hyperkalemia and 102 for leukopenia, with 12 and 7 patients requiring TMP-SMX cessation. In multivariate analysis, a living donor transplant protected against hyperkalemia (Odds Ratio 0.46, 95% CI 0.26-0.83, p < 0.01) while acute rejection risked leukopenia (Odds Ratio 3.31, 95% CI 1.39-7.90, p = 0.006).
TMP-SMX dose reduction is frequent in the first post-transplant year but PcP does not occur. To limit the need for TMP-SMX dose reduction due to adverse effects, a clinical trial comparing daily to thrice weekly single strength TMP-SMX in de-novo KTR is justified.
复方磺胺甲噁唑(TMP-SMX)是肾移植受者(KTR)预防卡氏肺孢子虫肺炎(PcP)的首选药物。移植后管理平衡了预防 PcP 和管理 TMP-SMX 相关不良反应的关系。TMP-SMX 剂量减少可解决不良反应问题,但对 PcP 发病的影响尚不清楚。
我们对 2011 年至 2015 年期间接受 TMP-SMX 单剂量每日预防 PcP 治疗 12 个月的所有移植患者进行了回顾性分析。记录实际 TMP-SMX 剂量和持续时间、不良反应、剂量减少次数和原因以及 PcP 事件。对与剂量减少相关的危险因素进行多变量逻辑回归分析。
在 438 名 KTR 中,233 名(53%)维持每日 TMP-SMX 治疗,205 名(47%)持续减少 1 次以上剂量,每日 TMP-SMX 减少剂量方案的点患病率在 18%至 25%之间。每日 TMP-SMX 的中位持续时间为 8.45/12 个月,贡献了 4137 个患者-月的每日 TMP-SMX 和 1110 个患者-月的减少剂量。任何患者均未发生 PcP。因高钾血症记录了 84 次剂量减少,因白细胞减少症记录了 102 次剂量减少,有 12 名和 7 名患者需要停止 TMP-SMX 治疗。多变量分析显示,活体供者移植可预防高钾血症(比值比 0.46,95%可信区间 0.26-0.83,p<0.01),而急性排斥反应则增加白细胞减少症风险(比值比 3.31,95%可信区间 1.39-7.90,p=0.006)。
TMP-SMX 剂量减少在移植后第一年很常见,但不会发生 PcP。为了减少因不良反应而减少 TMP-SMX 剂量的需求,有必要在初治 KTR 中比较每日一次与每周三次的单剂量 TMP-SMX 治疗的临床试验。