Division of Surgical Oncology, Department of Surgery, University of Tennessee Health Science Center, Memphis, TN, 38163, USA.
Department of Surgery, St Jude Children's Research Hospital, Memphis, TN, USA.
Ann Surg Oncol. 2020 Jan;27(1):171-178. doi: 10.1245/s10434-019-07339-2. Epub 2019 Apr 8.
Desmoplastic small round cell tumor (DSRCT) is a rare intra-abdominal soft tissue sarcoma affecting adolescents and young adults. Cytoreduction, hyperthermic intraperitoneal chemotherapy (CRS/HIPEC), and adjuvant radiotherapy may improve local control. We review our experience with patients who undergo CRS/HIPEC and adjuvant radiotherapy for DSRCT.
A retrospective review was performed for patients with DSRCT from 2013 to 2017 who underwent CRS/HIPEC. Clinicopathologic, operative, and outcome data were reviewed.
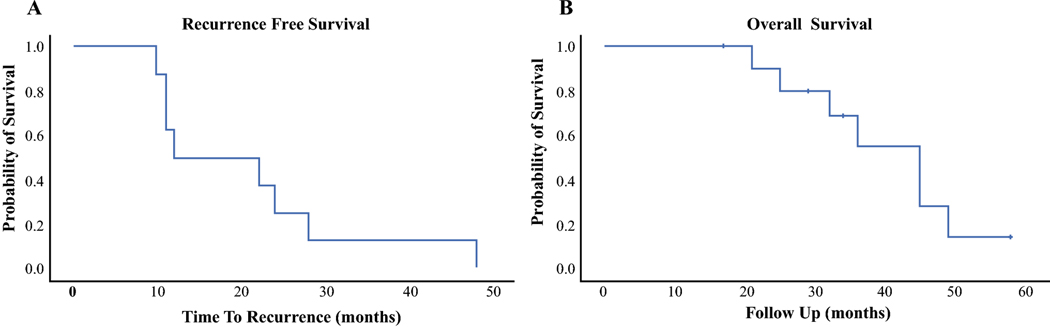
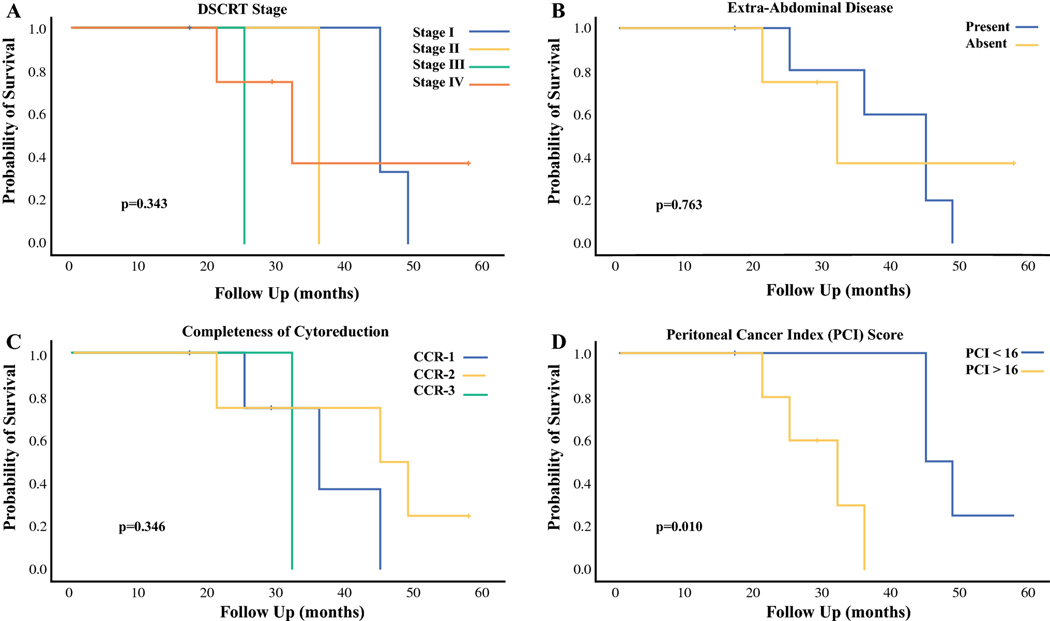
Ten CRS/HIPEC procedures were performed for nine patients (7 males, 6 Caucasian, median age 19 years (range 10-24)). Four patients presented with extra-abdominal disease; five had liver involvement. The median peritoneal cancer index was 16 (range 5-20). All received neoadjuvant chemotherapy. CCR 0/1 resection was possible in nine patients. Major complications occurred in four with no operative mortalities. All received adjuvant chemotherapy, seven received radiation therapy, and three received stem-cell transplant. All but one patient recurred after treatment. The median recurrence-free and overall survival (OS) were 12 and 45 months (95% confidence interval 35.1-54.9) respectively, with a 3-year OS of 55%. Long-term parenteral nutrition was required in eight for a median of 261 days (range 37-997). Clinically significant long-term complications requiring further surgery included gastroparesis (N = 1), small bowel obstruction (N = 3) and hemorrhagic cystitis (N = 2).
Multimodal therapy for DSRCT consisting of multiagent neoadjuvant chemotherapy, CRS/HIPEC, adjuvant chemotherapy, and radiation therapy is associated with potential cumulative toxicity. Recurrence after resection is common. Prolonged parenteral nutrition may be necessary, and late gastrointestinal and genitourinary complications may require additional treatment.
促纤维增生性小圆细胞肿瘤(DSRCT)是一种罕见的腹腔内软组织肉瘤,主要影响青少年和年轻成年人。细胞减灭术、腹腔内热灌注化疗(CRS/HIPEC)和辅助放疗可能有助于提高局部控制率。我们回顾了接受 CRS/HIPEC 和辅助放疗的 DSRCT 患者的经验。
对 2013 年至 2017 年期间接受 CRS/HIPEC 的 DSRCT 患者进行回顾性分析。回顾了临床病理、手术和结果数据。
共进行了 10 例 CRS/HIPEC 手术,9 例患者(7 例男性,6 例白种人,中位年龄 19 岁(范围 10-24 岁))。4 例患者有腹腔外疾病,5 例患者有肝转移。腹膜癌指数中位数为 16(范围 5-20)。所有患者均接受新辅助化疗。9 例患者达到 CCR 0/1 切除。4 例患者发生严重并发症,无手术死亡。所有患者均接受辅助化疗,7 例接受放疗,3 例接受干细胞移植。除 1 例患者外,所有患者均在治疗后复发。无复发生存和总生存(OS)中位数分别为 12 个月和 45 个月(95%置信区间 35.1-54.9),3 年 OS 率为 55%。8 例患者需要长期肠外营养,中位时间为 261 天(范围 37-997 天)。需要进一步手术的长期并发症包括胃轻瘫(1 例)、小肠梗阻(3 例)和出血性膀胱炎(2 例)。
多模式治疗 DSRCT 包括多药新辅助化疗、CRS/HIPEC、辅助化疗和放疗,可能会产生累积毒性。切除后复发很常见。可能需要长期肠外营养,晚期胃肠道和泌尿生殖系统并发症可能需要进一步治疗。