Humanitas University Gradenigo Hospital, 8 Corso Regina Margherita, 10132 Turin, Italy
Laboratory of Diabetes and Metabolic Disorders, Department of Medical Sciences, University of Turin, Turin, Italy.
BMJ. 2019 Apr 9;365:l1328. doi: 10.1136/bmj.l1328.
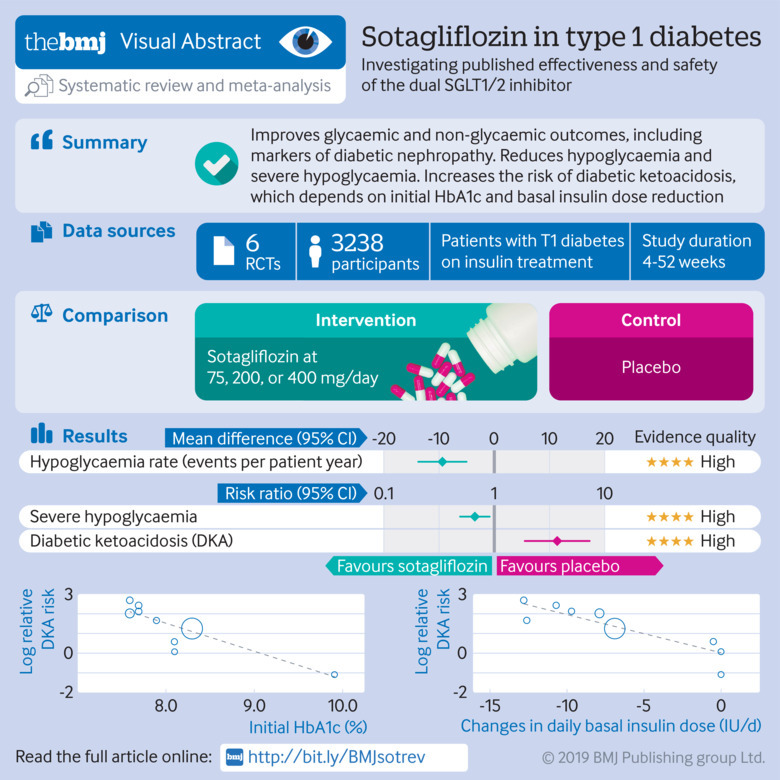
To assess the efficacy and safety of dual sodium glucose cotransporter (SGLT) 1/2 inhibitor sotagliflozin in type 1 diabetes mellitus.
Meta-analysis of randomised controlled trials.
Medline; Cochrane Library; Embase; international meeting abstracts; international and national clinical trial registries; and websites of US, European, and Japanese regulatory authorities, up to 10 January 2019.
Randomised controlled trials evaluating the effect of sotagliflozin versus active comparators or placebo on glycaemic and non-glycaemic outcomes and on adverse events in type 1 diabetes in participants older than 18. Three reviewers extracted data for study characteristics, outcomes of interest, and risk of bias and summarised strength of evidence using the grading of recommendations assessment, development, and evaluation approach. Main outcomes were pooled using random effects models.
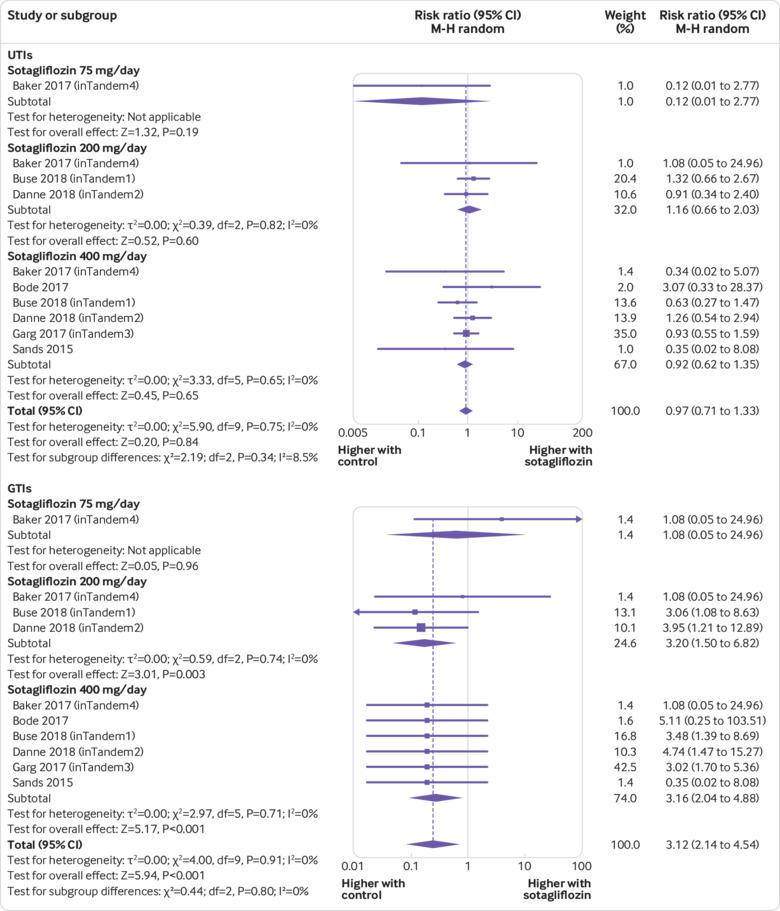
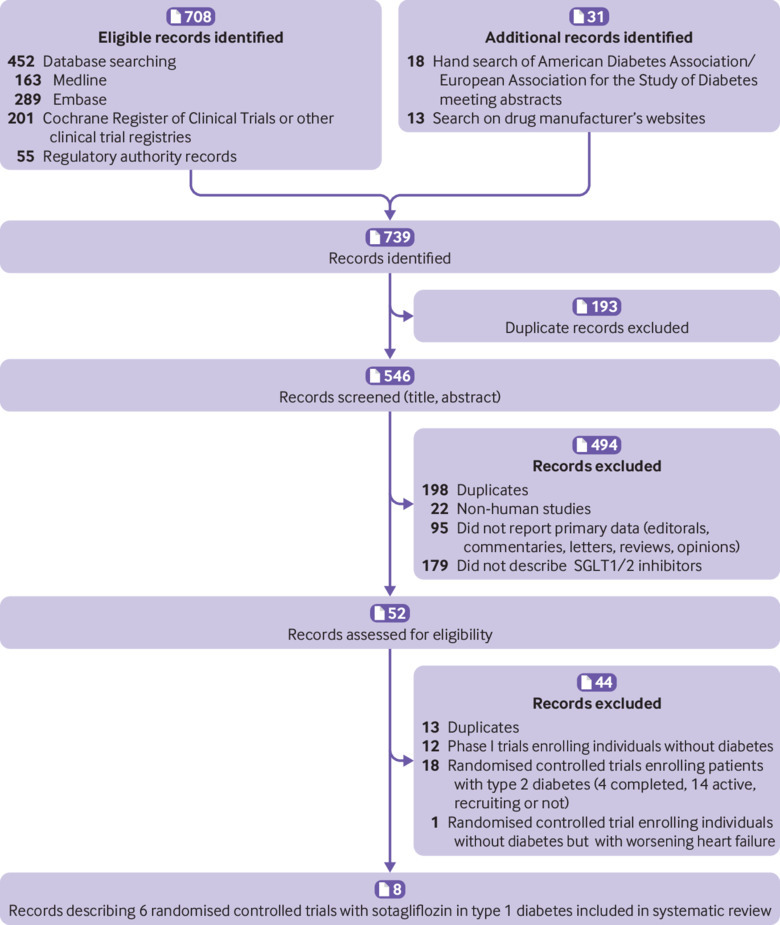
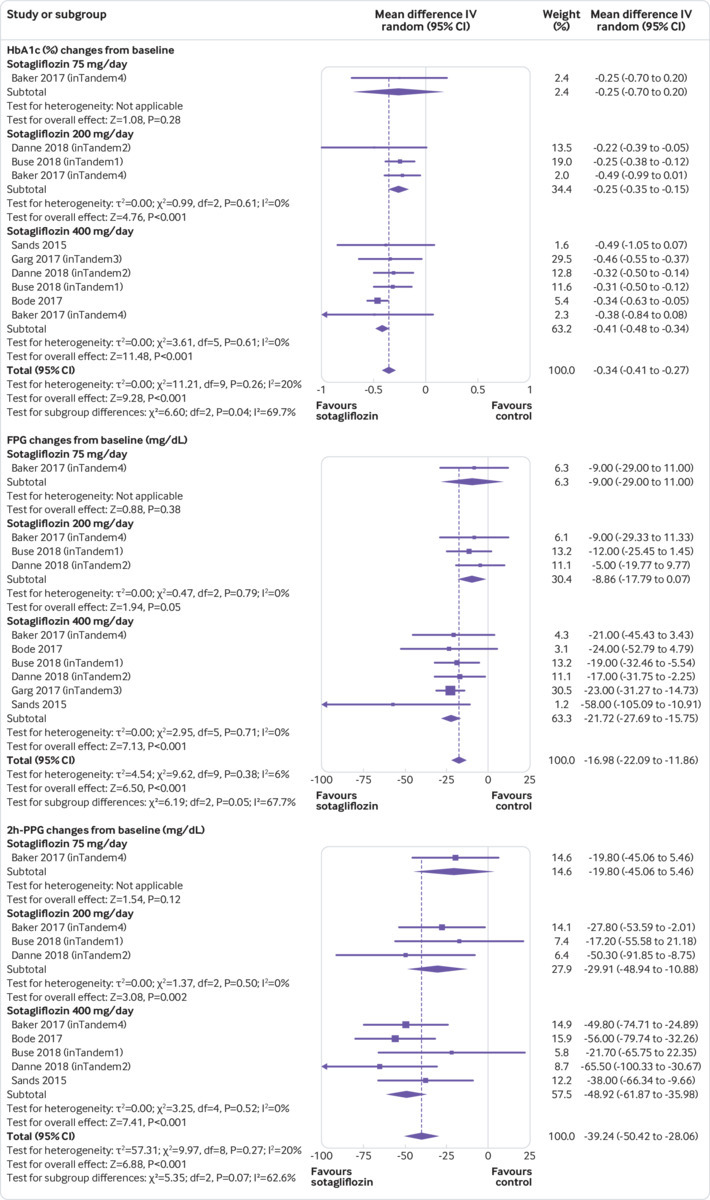
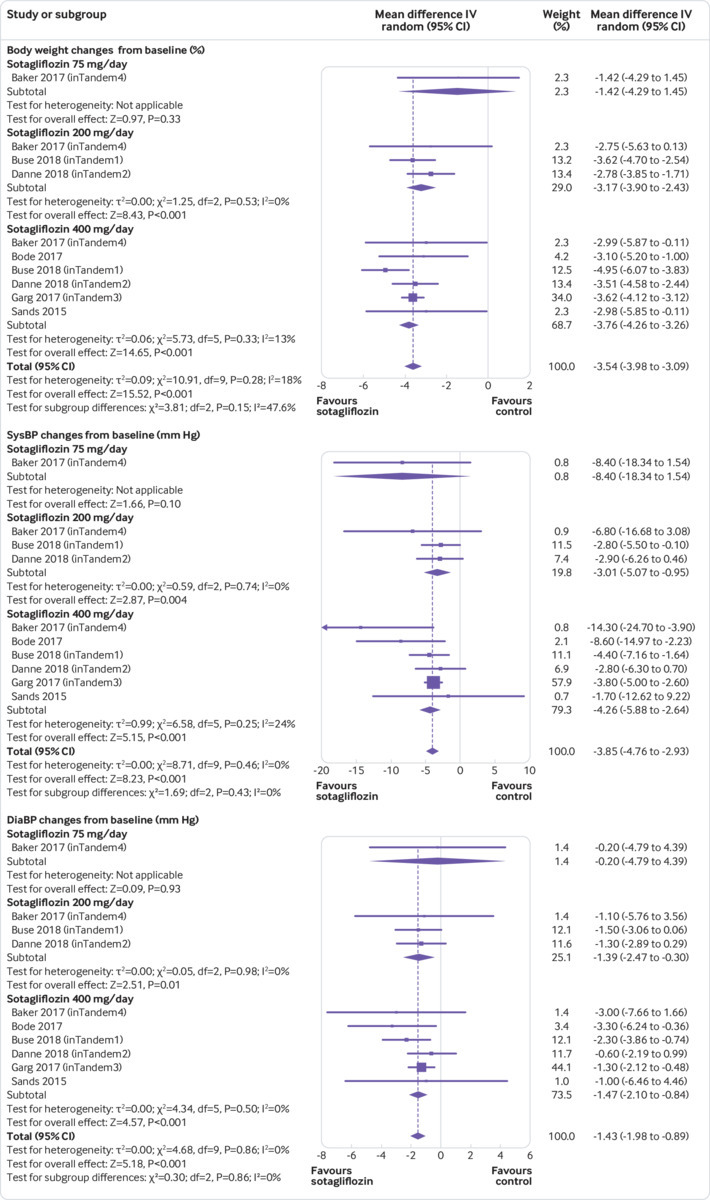
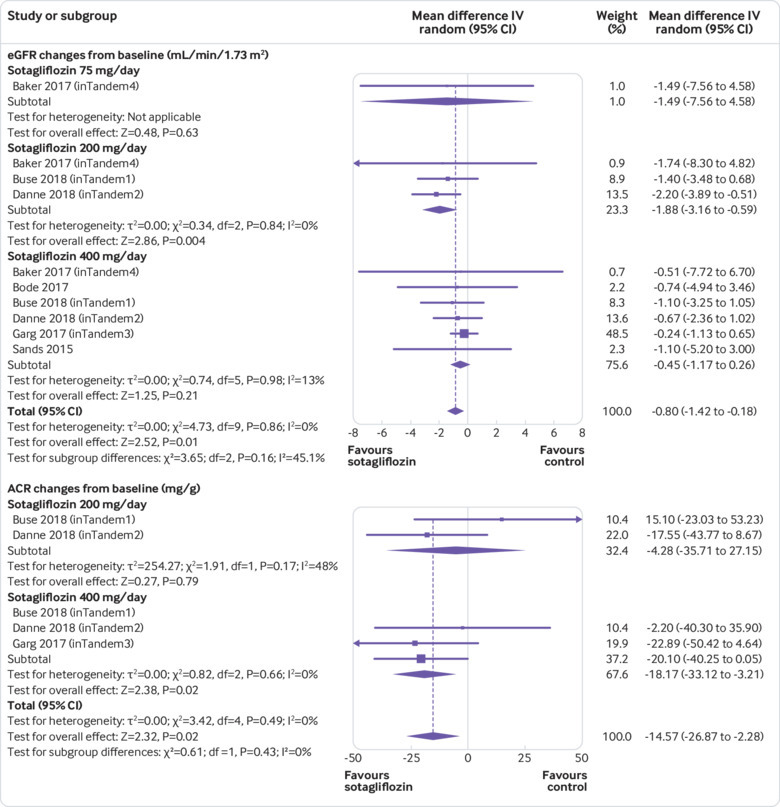
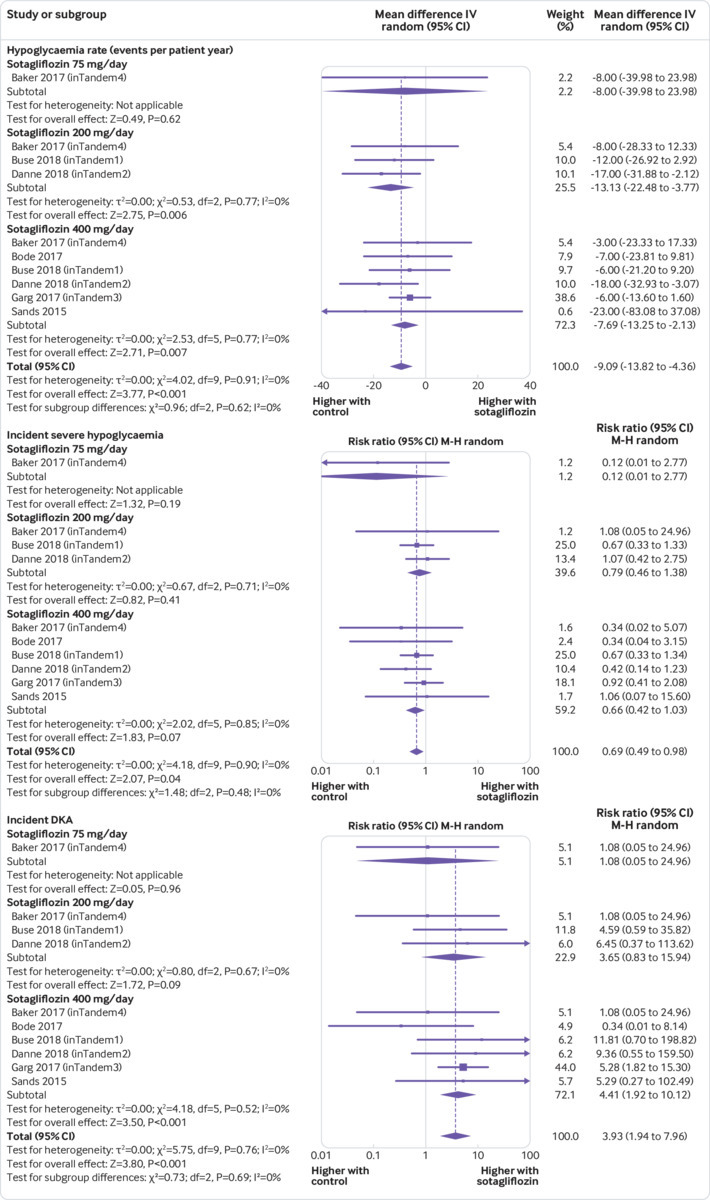
Of 739 records identified, six randomised placebo controlled trials (n=3238, duration 4-52 weeks) were included. Sotagliflozin reduced levels of glycated haemoglobin (HbA1c; weighted mean difference -0.34% (95% confidence interval -0.41% to -0.27%), P<0.001); fasting plasma glucose (-16.98 mg/dL, -22.1 to -11.9; 1 mg/dL=0.0555 mmol/L) and two hour-postprandial plasma glucose (-39.2 mg/dL, -50.4 to -28.1); and daily total, basal, and bolus insulin dose (-8.99%, -10.93% to -7.05%; -8.03%, -10.14% to -5.93%; -9.14%, -12.17% to -6.12%; respectively). Sotagliflozin improved time in range (weighted mean difference 9.73%, 6.66% to 12.81%) and other continuous glucose monitoring parameters, and reduced body weight (-3.54%, -3.98% to -3.09%), systolic blood pressure (-3.85 mm Hg, -4.76 to -2.93), and albuminuria (albumin:creatinine ratio -14.57 mg/g, -26.87 to -2.28). Sotagliflozin reduced hypoglycaemia (weighted mean difference -9.09 events per patient year, -13.82 to -4.36) and severe hypoglycaemia (relative risk 0.69, 0.49 to 0.98). However, the drug increased the risk of ketoacidosis (relative risk 3.93, 1.94 to 7.96), genital tract infections (3.12, 2.14 to 4.54), diarrhoea (1.50, 1.08 to 2.10), and volume depletion events (2.19, 1.10 to 4.36). Initial HbA1c and basal insulin dose adjustment were associated with the risk of diabetic ketoacidosis. A sotagliflozin dose of 400 mg/day was associated with a greater improvement in most glycaemic and non-glycaemic outcomes than the 200 mg/day dose, without increasing the risk of adverse events. The quality of evidence was high to moderate for most outcomes, but low for major adverse cardiovascular events and all cause death. The relatively short duration of trials prevented assessment of long term outcomes.
In type 1 diabetes, sotagliflozin improves glycaemic and non-glycaemic outcomes and reduces hypoglycaemia rate and severe hypoglycaemia. The risk of diabetic ketoacidosis could be minimised by appropriate patient selection and down-titration of the basal insulin dose.
评估双重钠-葡萄糖共转运蛋白(SGLT)1/2 抑制剂索格列净在 1 型糖尿病中的疗效和安全性。
随机对照试验的荟萃分析。
Medline;Cochrane 图书馆;Embase;国际会议摘要;国际和国家临床试验注册处;以及美国、欧洲和日本监管机构的网站,截至 2019 年 1 月 10 日。
评估索格列净与活性对照或安慰剂在 18 岁以上参与者中对血糖和非血糖结局以及不良事件的影响的随机对照试验。三位评审员提取了研究特征、感兴趣的结局以及偏倚风险的数据,并使用推荐评估、制定和评估方法(Grading of Recommendations Assessment, Development, and Evaluation approach)评估证据的强度。使用随机效应模型汇总主要结局。
在 739 条记录中,有 6 项随机安慰剂对照试验(n=3238,持续时间 4-52 周)被纳入。索格列净降低糖化血红蛋白(HbA1c;加权均数差-0.34%(95%置信区间-0.41%至-0.27%),P<0.001);空腹血糖(-16.98 mg/dL,-22.1 至-11.9;1 mg/dL=0.0555 mmol/L)和餐后 2 小时血糖(-39.2 mg/dL,-50.4 至-28.1);以及每日总、基础和餐时胰岛素剂量(-8.99%,-10.93%至-7.05%;-8.03%,-10.14%至-5.93%;-9.14%,-12.17%至-6.12%;分别)。索格列净改善了时间在范围内(加权均数差 9.73%,6.66%至 12.81%)和其他连续血糖监测参数,并降低了体重(-3.54%,-3.98%至-3.09%)、收缩压(-3.85 mmHg,-4.76 至-2.93)和白蛋白尿(白蛋白:肌酐比值-14.57 mg/g,-26.87 至-2.28)。索格列净降低了低血糖(加权均数差-9.09 个患者年事件,-13.82 至-4.36)和严重低血糖(相对风险 0.69,0.49 至 0.98)的风险。然而,该药物增加了酮症酸中毒(相对风险 3.93,1.94 至 7.96)、生殖道感染(3.12,2.14 至 4.54)、腹泻(1.50,1.08 至 2.10)和容量缺失事件(2.19,1.10 至 4.36)的风险。初始 HbA1c 和基础胰岛素剂量调整与糖尿病酮症酸中毒的风险相关。与 200 mg/天剂量相比,索格列净 400 mg/天的剂量可更显著改善大多数血糖和非血糖结局,而不会增加不良事件的风险。大多数结局的证据质量为高到中度,但主要不良心血管事件和全因死亡的证据质量为低。试验的持续时间相对较短,无法评估长期结局。
在 1 型糖尿病中,索格列净改善血糖和非血糖结局,并降低低血糖发生率和严重低血糖发生率。通过适当的患者选择和基础胰岛素剂量的下调,可以最大限度地降低糖尿病酮症酸中毒的风险。