Saraireh Hamzeh, Tayyem Obada, Siddiqui Mohamed Tausif, Hmoud Bashar, Bilal Mohammad
Department of Internal Medicine, University of Texas Medical Branch, Galveston, TX, USA.
Department of Internal Medicine, New York Medical College, Valhalla, NY, USA.
Gastroenterol Rep (Oxf). 2019 Apr;7(2):115-120. doi: 10.1093/gastro/goy031. Epub 2018 Aug 16.
Diverticular bleeding (DB) is the most common cause of severe acute lower gastrointestinal bleeding (GIB) in developed countries. The role of early colonoscopy (<24 hours) continues to remain controversial and data on early colonoscopy in acute DB are scant. We aimed to evaluate the effect of timing of colonoscopy on outcomes in patients with acute DB using a nationwide inpatient sample.
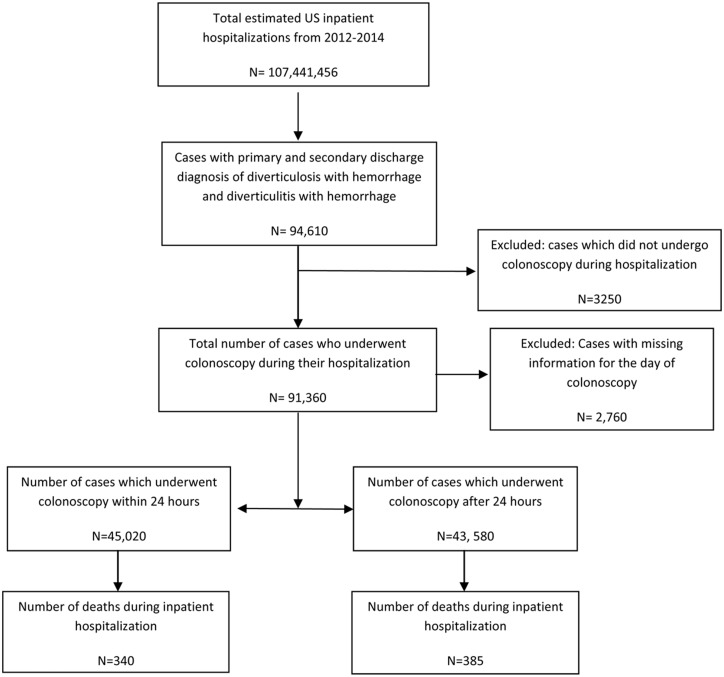
Data from the nationwide inpatient sample from 2012 to 2014 were used. The ninth version of the International Classification of Diseases coding system ICD 9 was used for patient selection. We included discharges with the primary and secondary inpatient diagnosis of diverticulosis with bleeding and diverticulitis with bleeding. Discharges with no primary or secondary diagnosis of diverticulosis with bleeding, diverticulitis with bleeding, patients who were less than 18 years old and those who did not undergo colonoscopy during the admission were excluded. The primary outcomes were length of stay (LOS) and total hospitalization costs.
A total of 88 600 patients were included in our analysis, amongst whom 45 020 (50.8%) had colonoscopy within 24 hours of admission (early colonoscopy), while 43 580 (49.2%) patients had colonoscopy after 24 hours of admission (late colonoscopy). LOS was significantly lower in patients with early colonoscopy as compared to those with late colonoscopy (3.7 vs 5.6 days, < 0.0001). Total hospitalization costs were also significantly lower in patients with early colonoscopy ($9317 vs $11 767, < 0.0001). There was no difference in mortality between both groups (0.7 vs 0.8%). After adjusting for potential confounders, the differences in LOS and total hospitalization costs between early and late colonoscopy remained statistically significant.
Early colonoscopy in acute DB significantly reduced LOS and total hospitalization costs. There was no significant difference in mortality observed. Performance of early colonoscopy in the appropriate patients presenting with acute DB can have potential cost-saving implications. Further research is needed to identify which patients would benefit from early colonoscopy in DB.
在发达国家,憩室出血(DB)是严重急性下消化道出血(GIB)的最常见原因。早期结肠镜检查(<24小时)的作用仍存在争议,且关于急性DB早期结肠镜检查的数据很少。我们旨在使用全国住院患者样本评估结肠镜检查时机对急性DB患者预后的影响。
使用2012年至2014年全国住院患者样本的数据。采用国际疾病分类编码系统ICD 9第九版进行患者选择。我们纳入了以憩室病伴出血和憩室炎伴出血作为主要和次要住院诊断的出院病例。排除没有憩室病伴出血、憩室炎伴出血的主要或次要诊断的出院病例、年龄小于18岁的患者以及住院期间未接受结肠镜检查的患者。主要结局为住院时间(LOS)和总住院费用。
我们的分析共纳入88600例患者,其中45020例(50.8%)在入院后24小时内接受了结肠镜检查(早期结肠镜检查),而43580例(49.2%)患者在入院24小时后接受了结肠镜检查(晚期结肠镜检查)。与晚期结肠镜检查患者相比,早期结肠镜检查患者的LOS显著更低(3.7天对5.6天,<0.0001)。早期结肠镜检查患者的总住院费用也显著更低(9317美元对11767美元,<0.0001)。两组之间的死亡率没有差异(0.7%对0.8%)。在调整潜在混杂因素后,早期和晚期结肠镜检查之间LOS和总住院费用的差异仍具有统计学意义。
急性DB患者早期结肠镜检查可显著降低LOS和总住院费用。未观察到死亡率有显著差异。对出现急性DB的合适患者进行早期结肠镜检查可能具有潜在的成本节约意义。需要进一步研究以确定哪些患者将从DB早期结肠镜检查中获益。