Division of Nephrology, Ichiyokai Harada Hospital, 7-10 Kairoyama-cho, Saeki-ku, Hiroshima, 731-5134, Japan.
Ichiyokai Ichiyokai Clinic, 10-3 Asahien, Saeki-ku, Hiroshima, 731-5133, Japan.
Int Urol Nephrol. 2019 Jun;51(6):1043-1052. doi: 10.1007/s11255-019-02073-w. Epub 2019 Apr 11.
It is unclear whether hypomagnesemia is an independent risk factor or innocent bystander for mortality in maintenance hemodialysis (MHD) patients. Thus, we studied associations between hypomagnesemia and all-cause as well as cardiovascular (CV) mortality in MHD patients.
Baseline clinical characteristics and coronary artery calcium score (CACS) of 353 Japanese MHD patients were reviewed. Three-year survival rate and mortality risk factors were assessed.
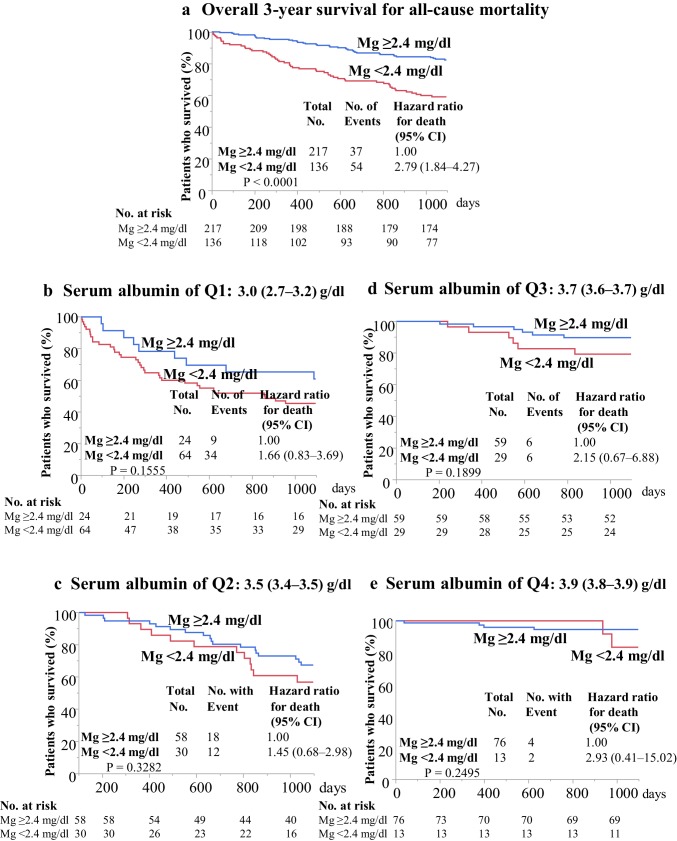
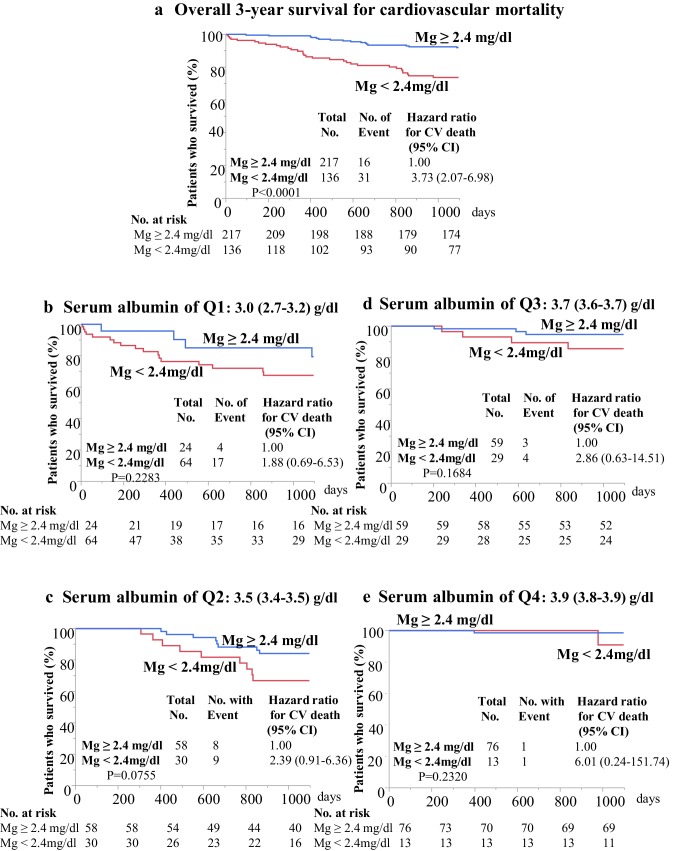
Median (interquartile range) age, dialysis vintage, serum magnesium (Mg), serum albumin and CACS of the subjects were 68 (60-78) years, 75 (32-151) months, 2.4 (2.2-2.7) mg/dl, 3.6 (3.3-3.8) g/dl, and 1181 (278-3190), respectively. During the 3-year period, 91 patients died. Kaplan-Meier overall 3-year survival rates were 59.0% in in patients with Mg < 2.4 mg/dl (n = 136) and 82.3% in patients with Mg ≥ 2.4 mg/dl (n = 217), (P < 0.0001). In Cox regression models not incorporating serum albumin, Mg < 2.4 mg/dl was significantly associated with 3-year all-cause death, independent of age, dialysis vintage, average ultrafiltration, Log (CACS + 1), warfarin use, serum potassium, high-sensitivity C-reactive protein (hsCRP), phosphate, uric acid, and intact parathyroid hormone [Hazard ratio (HR) 95% confidence interval (CI): 2.82 (1.31-6.29), P = 0.0078], and CV death, independent of age, dialysis vintage, Log (CACS + 1), warfarin use, serum hsCRP, and uric acid [HR (95% CI): 4.47 (1.45-16.76), P = 0.0086]. Nevertheless, associations of Mg < 2.4 mg/dl with all-cause and CV mortality were all absent in models that included serum albumin.
Hypomagnesemia is not an independent risk factor for mortality but is associated with malnutrition in MHD patients.
低镁血症是否是维持性血液透析(MHD)患者死亡的独立危险因素或无辜旁观者尚不清楚。因此,我们研究了低镁血症与 MHD 患者全因和心血管(CV)死亡率之间的关系。
回顾了 353 名日本 MHD 患者的基线临床特征和冠状动脉钙评分(CACS)。评估了 3 年生存率和死亡风险因素。
研究对象的中位(四分位距)年龄、透析年限、血清镁(Mg)、血清白蛋白和 CACS 分别为 68(60-78)岁、75(32-151)个月、2.4(2.2-2.7)mg/dl、3.6(3.3-3.8)g/dl 和 1181(278-3190)。在 3 年期间,有 91 名患者死亡。Kaplan-Meier 总体 3 年生存率在 Mg<2.4mg/dl(n=136)的患者中为 59.0%,在 Mg≥2.4mg/dl(n=217)的患者中为 82.3%(P<0.0001)。在未纳入血清白蛋白的 Cox 回归模型中,Mg<2.4mg/dl 与 3 年全因死亡相关,与年龄、透析年限、平均超滤量、Log(CACS+1)、华法林使用、血清钾、高敏 C 反应蛋白(hsCRP)、磷酸盐、尿酸和完整甲状旁腺激素独立相关[风险比(HR)95%置信区间(CI):2.82(1.31-6.29),P=0.0078],与 CV 死亡相关,与年龄、透析年限、Log(CACS+1)、华法林使用、血清 hsCRP 和尿酸独立相关[HR(95%CI):4.47(1.45-16.76),P=0.0086]。然而,在包括血清白蛋白的模型中,Mg<2.4mg/dl 与全因和 CV 死亡率的关联均不存在。
低镁血症不是死亡的独立危险因素,但与 MHD 患者的营养不良有关。