Jansen Christian, Schröder Anna, Schueler Robert, Lehmann Jennifer, Praktiknjo Michael, Uschner Frank E, Schierwagen Robert, Thomas Daniel, Monteiro Sofia, Nickenig Georg, Strassburg Christian P, Meyer Carsten, Arroyo Vicente, Hammerstingl Christoph, Trebicka Jonel
Department of Internal Medicine I University Clinic Bonn Bonn Germany.
Department of Internal Medicine II University Clinic Bonn Bonn Germany.
Hepatol Commun. 2019 Jan 22;3(3):340-347. doi: 10.1002/hep4.1308. eCollection 2019 Mar.
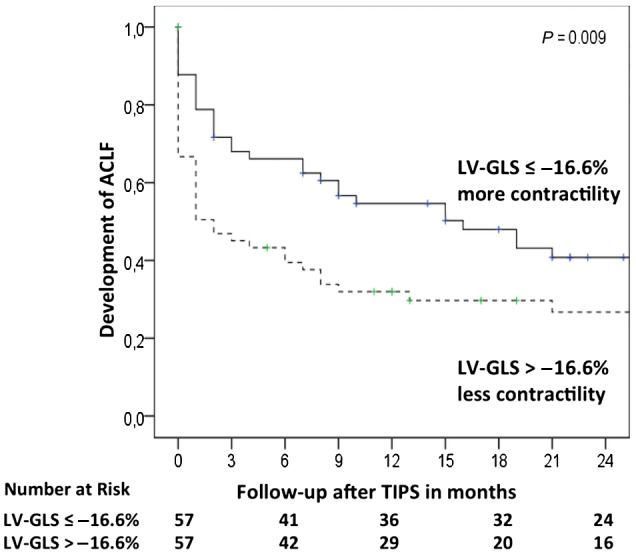
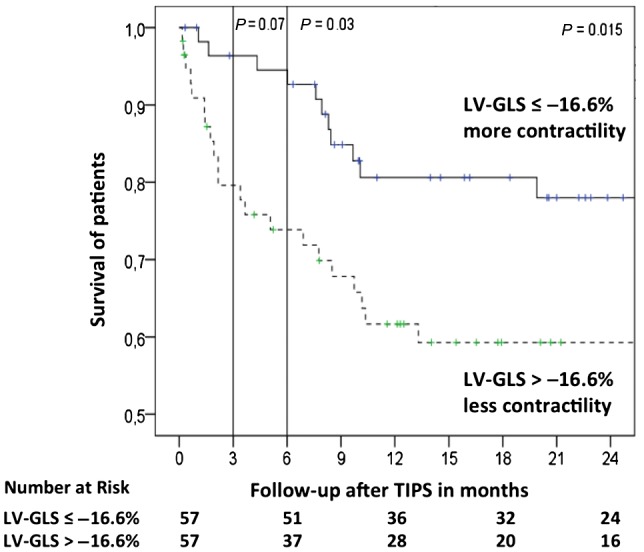
Acute deterioration of liver cirrhosis (e.g., infections, acute-on-chronic liver failure [ACLF]) requires an increase in cardiac contractility. The insufficiency to respond to these situations could be deleterious. Left ventricular global longitudinal strain (LV-GLS) has been shown to reflect left cardiac contractility in cirrhosis better than other parameters and might bear prognostic value. Therefore, this retrospective study investigated the role of LV-GLS in the outcome after transjugular intrahepatic portosystemic shunt (TIPS) and the development of ACLF. We included 114 patients (48 female patients) from the Noninvasive Evaluation Program for TIPS and Their Follow-Up Network (NEPTUN) cohort. This number provided sufficient quality and structured follow-up with the possibility of calculating major scores (Child, Model for End-Stage Liver Disease [MELD], Chronic Liver Failure Consortium acute decompensation [CLIF-C AD] scores) and recording of the events (development of decompensation episode and ACLF). We analyzed the association of LV-GLS with overall mortality and development of ACLF in patients with TIPS. LV-GLS was independently associated with overall mortality (hazard ratio [HR], 1.123; 95% confidence interval [CI],1.010-1.250) together with aspartate aminotransferase (HR, 1.009; 95% CI, 1.004-1.014) and CLIF-C AD score (HR, 1.080; 95% CI, 1.018-1.137). Area under the receiver operating characteristic curve (AUROC) analysis for LV-GLS for overall survival showed higher area under the curve (AUC) than MELD and CLIF-C AD scores (AUC, 0.688 versus 0.646 and 0.573, respectively). The best AUROC-determined LV-GLS cutoff was -16.6% to identify patients with a significantly worse outcome after TIPS at 3 months, 6 months, and overall. LV-GLS was independently associated with development of ACLF (HR, 1.613; 95% CI, 1.025-2.540) together with a MELD score above 15 (HR, 2.222; 95% CI, 1.400-3.528). LV-GLS is useful for identifying patients at risk of developing ACLF and a worse outcome after TIPS. Although validation is required, this tool might help to stratify risk in patients receiving TIPS.
肝硬化急性恶化(如感染、慢加急性肝衰竭[ACLF])需要增强心脏收缩力。应对这些情况的能力不足可能是有害的。左心室整体纵向应变(LV-GLS)已被证明比其他参数更能反映肝硬化患者的左心收缩力,且可能具有预后价值。因此,这项回顾性研究调查了LV-GLS在经颈静脉肝内门体分流术(TIPS)后结局及ACLF发生中的作用。我们纳入了经颈静脉肝内门体分流术及其随访网络(NEPTUN)队列中的114例患者(48例女性患者)。这个样本量提供了足够的质量和结构化随访,有计算主要评分(Child、终末期肝病模型[MELD]、慢性肝衰竭联盟急性失代偿[CLIF-C AD]评分)的可能,并记录事件(失代偿发作和ACLF的发生)。我们分析了LV-GLS与TIPS患者的全因死亡率及ACLF发生之间的关联。LV-GLS与全因死亡率独立相关(风险比[HR],1.123;95%置信区间[CI],1.010 - 1.250),同时与天冬氨酸转氨酶(HR,1.009;95% CI,1.004 - 1.014)及CLIF-C AD评分(HR,1.080;95% CI,1.018 - 1.137)相关。LV-GLS对总体生存的受试者工作特征曲线下面积(AUROC)分析显示曲线下面积(AUC)高于MELD和CLIF-C AD评分(AUC分别为0.688、0.646和0.573)。由AUROC确定的LV-GLS最佳截断值为-16.6%,以识别TIPS术后3个月、6个月及总体结局显著更差的患者。LV-GLS与ACLF的发生独立相关(HR,1.613;95% CI,1.025 - 2.540),同时与MELD评分高于15相关(HR,2.222;95% CI,1.400 - 3.528)。LV-GLS有助于识别有发生ACLF风险及TIPS术后结局较差的患者。尽管需要验证,但该工具可能有助于对接受TIPS的患者进行风险分层。