Rao P Syamasundar
University of Texas-Houston McGovern Medical School, Children's Memorial Hermann Hospital, Houston, TX 77030, USA.
Children (Basel). 2019 Apr 4;6(4):54. doi: 10.3390/children6040054.
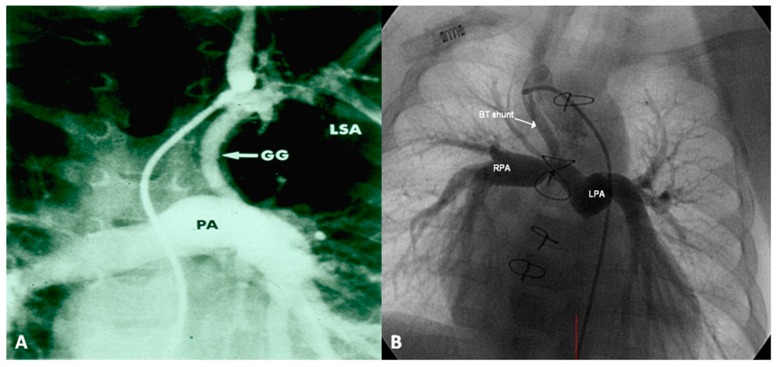
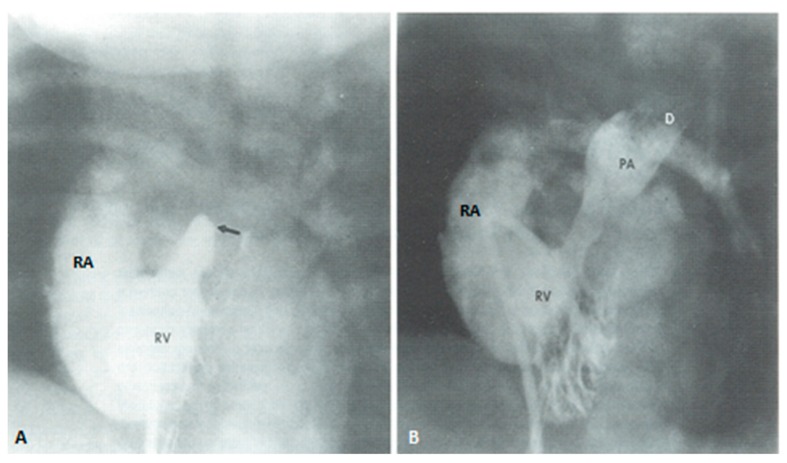
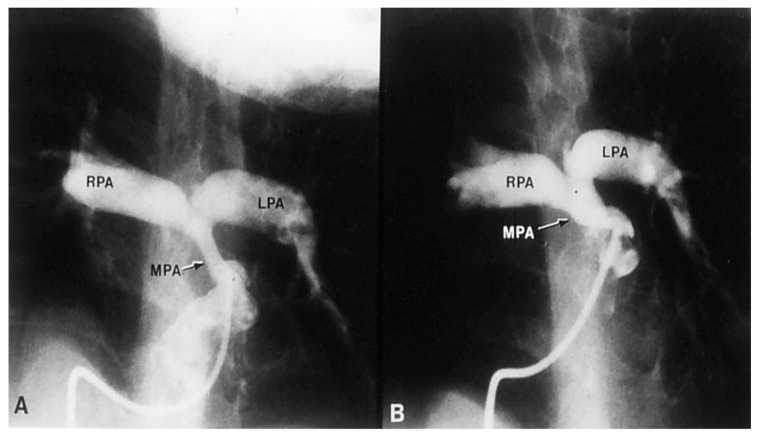
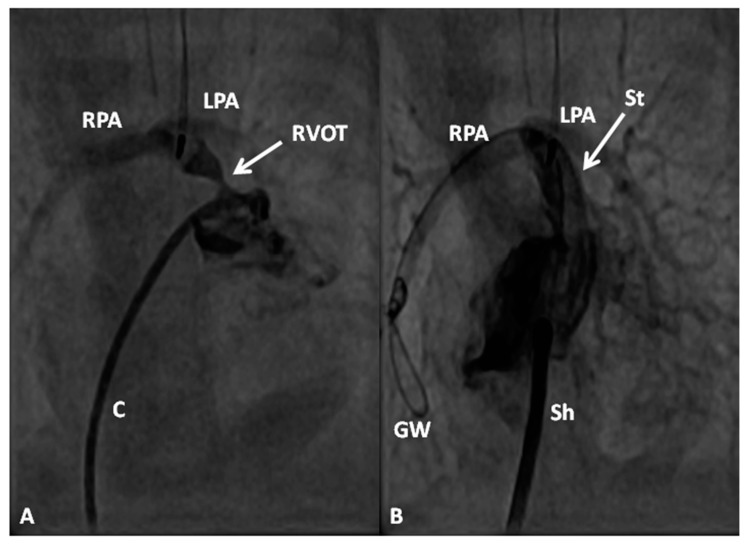
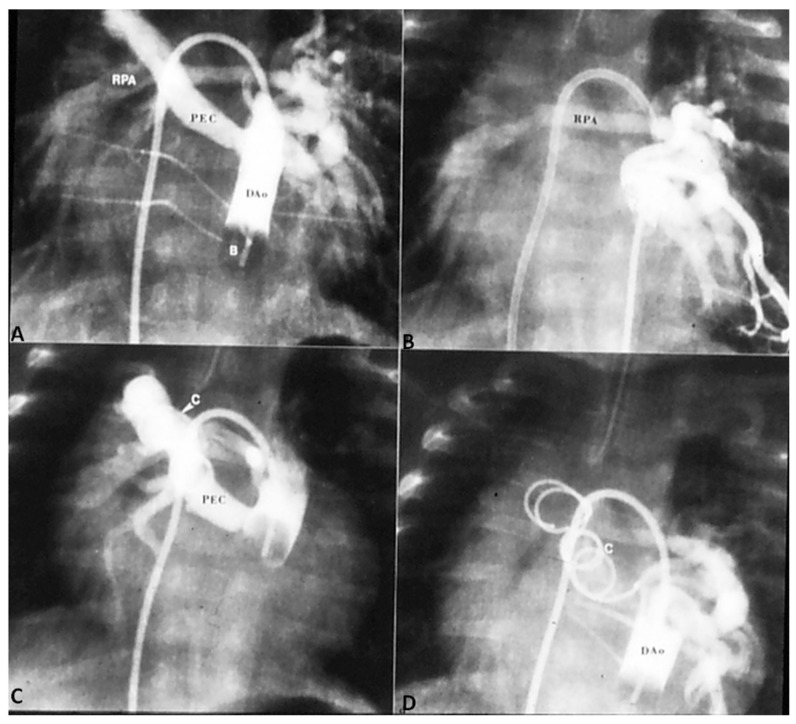
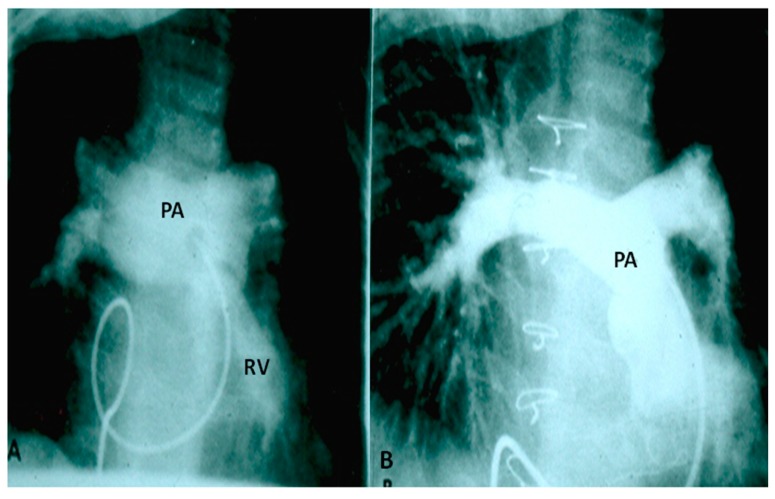
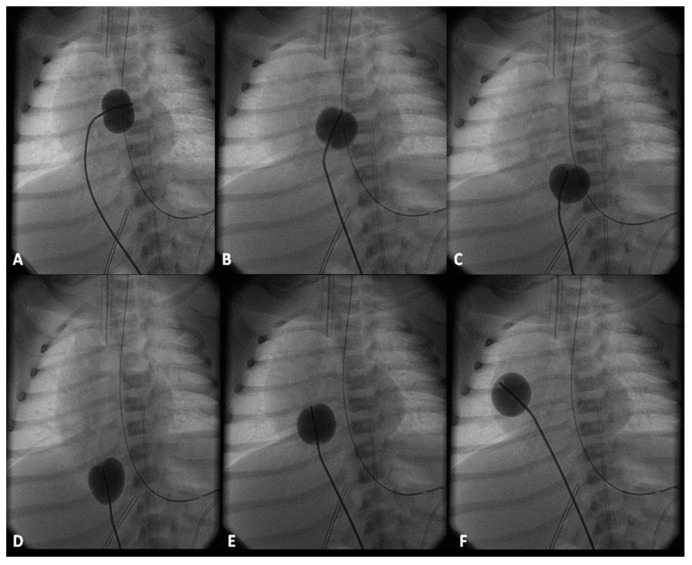
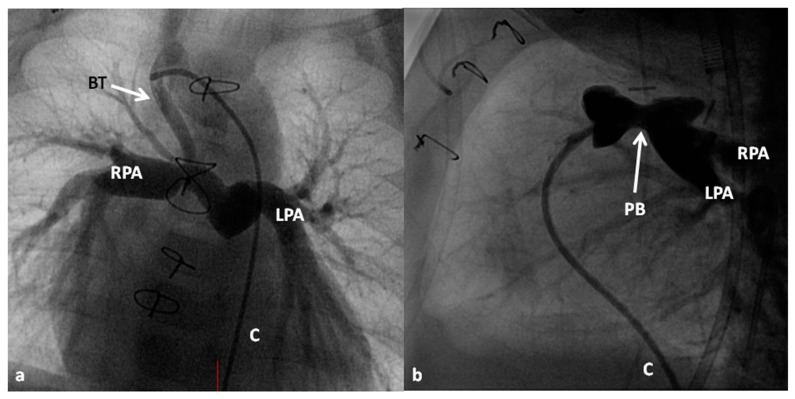
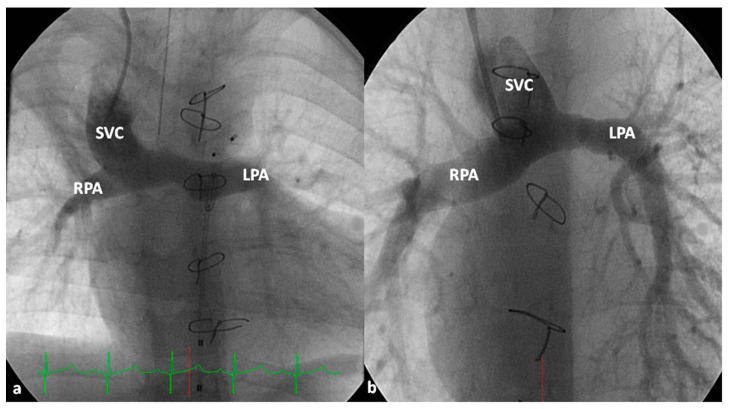
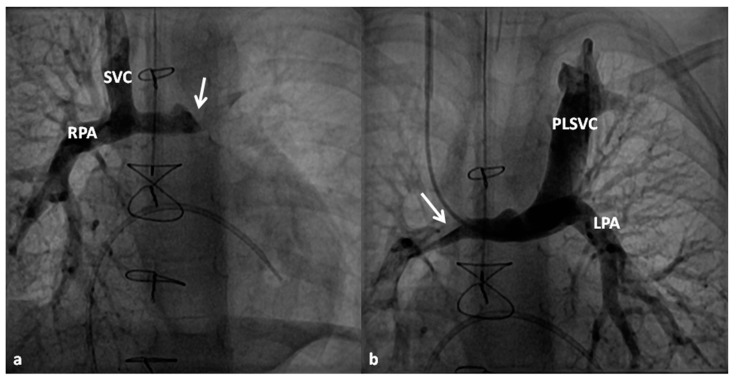
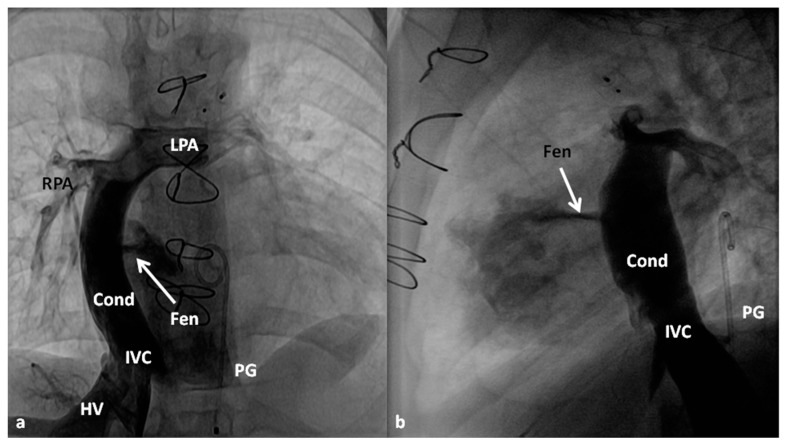
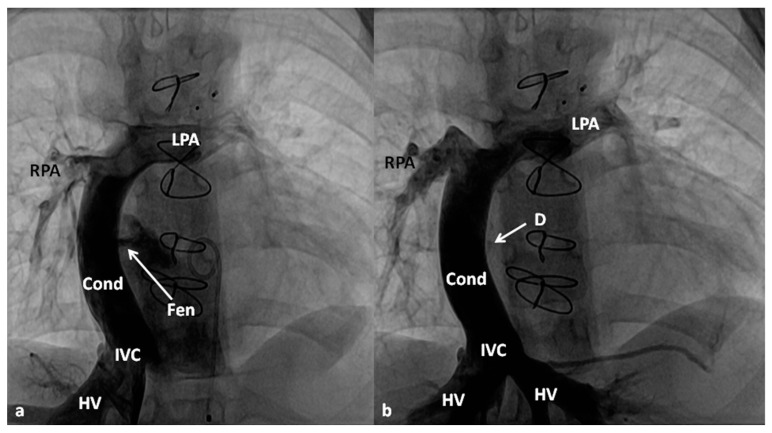
In this review management of the most common cyanotic congenital heart defects (CHDs) was discussed; the management of acyanotic CHD was reviewed in Part I of this series. While the need for intervention in acyanotic CHD is by and large determined by the severity of the lesion, most cyanotic CHDs require intervention, mostly by surgery. Different types of tetralogy of Fallot require different types of total surgical corrective procedures, and some may require initial palliation, mainly by modified Blalock-Taussig shunts. Babies with transposition of the great arteries with an intact ventricular septum as well as those with ventricular septal defects (VSD) need an arterial switch (Jatene) procedure while those with both VSD and pulmonary stenosis should be addressed by Rastelli procedure. These procedures may need to be preceded by prostaglandin infusion and/or balloon atrial septostomy in some babies. Infants with tricuspid atresia require initial palliation either with a modified Blalock-Taussig shunt or banding of the pulmonary artery and subsequent staged Fontan (bidirectional Glenn and fenestrated Fontan with extra-cardiac conduit). Neonates with total anomalous pulmonary venous connection are managed by anastomosis of the common pulmonary vein with the left atrium either electively in non-obstructed types or as an emergency procedure in the obstructed types. Babies with truncus arteriosus are treated by surgical closure of VSD along with right ventricle to pulmonary artery conduit. The other defects, namely, hypoplastic left heart syndrome, pulmonary atresia with intact ventricular septum, double-outlet right ventricle, double-inlet left ventricle and univentricular hearts largely require multistage surgical correction. The currently existing medical, trans-catheter and surgical techniques to manage cyanotic CHD are safe and effective and can be performed at a relatively low risk.
在本综述中,讨论了最常见的青紫型先天性心脏病(CHD)的管理;本系列第一部分回顾了非青紫型CHD的管理。虽然非青紫型CHD干预的必要性大体上由病变的严重程度决定,但大多数青紫型CHD需要干预,主要是通过手术。不同类型的法洛四联症需要不同类型的完全手术矫正程序,有些可能需要初始姑息治疗,主要是通过改良的布莱洛克 - 陶西格分流术。室间隔完整的大动脉转位婴儿以及室间隔缺损(VSD)婴儿需要进行动脉调转术(贾滕手术),而同时患有VSD和肺动脉狭窄的婴儿应采用拉斯泰利手术治疗。在一些婴儿中,这些手术可能需要在前列环素输注和/或球囊房间隔造口术之前进行。三尖瓣闭锁的婴儿需要初始姑息治疗,要么采用改良的布莱洛克 - 陶西格分流术,要么对肺动脉进行束带术,随后进行分期的方坦手术(双向格林手术和带心外管道的开窗方坦手术)。完全性肺静脉异位连接的新生儿,对于非梗阻型可择期进行共同肺静脉与左心房吻合术,对于梗阻型则作为急诊手术进行处理。永存动脉干的婴儿通过手术闭合VSD并同时进行右心室至肺动脉管道治疗。其他缺陷,即左心发育不全综合征、室间隔完整的肺动脉闭锁、右心室双出口、左心室双入口和单心室心脏,大多需要多阶段手术矫正。目前现有的用于管理青紫型CHD的医学、经导管和手术技术是安全有效的,并且可以在相对较低的风险下进行。