Gustave Roussy, Service de Biostatistiques et d'Épidémiologie and Ligue Nationale Contre le Cancer Meta-Analysis Platform, Université Paris-Saclay, F-94805, Villejuif, France.
Centre for Research in Epidemiology and Population Health, INSERM U1018, Paris-Saclay University, Villejuif, France.
Syst Rev. 2019 Apr 15;8(1):96. doi: 10.1186/s13643-019-0984-x.
This study aimed at applying the restricted mean survival time difference (rmstD) as an absolute outcome measure in a network meta-analysis and comparing the results with those obtained using hazard ratios (HR) from the individual patient data (IPD) network meta-analysis (NMA) on the role of chemotherapy for nasopharyngeal carcinoma (NPC) recently published by the MAC-NPC collaborative group (Meta-Analysis of Chemotherapy [CT] in NPC).
Twenty trials (5144 patients) comparing radiotherapy (RT) with or without CT in non-metastatic NPC were included. Treatments were grouped in seven categories: RT alone (RT), induction CT followed by RT (IC-RT), RT followed by adjuvant CT (RT-AC), IC followed by RT followed by AC (IC-RT-AC), concomitant chemoradiotherapy (CRT), IC followed by CRT (IC-CRT), and CRT followed by AC (CRT-AC). The primary endpoint was overall survival (OS); secondary endpoints were progression-free survival and locoregional control. The rmstD was estimated at t* = 10 years in each trial. Random-effect frequentist NMA models were applied. P score was used to rank treatments. Heterogeneity and inconsistency were evaluated.
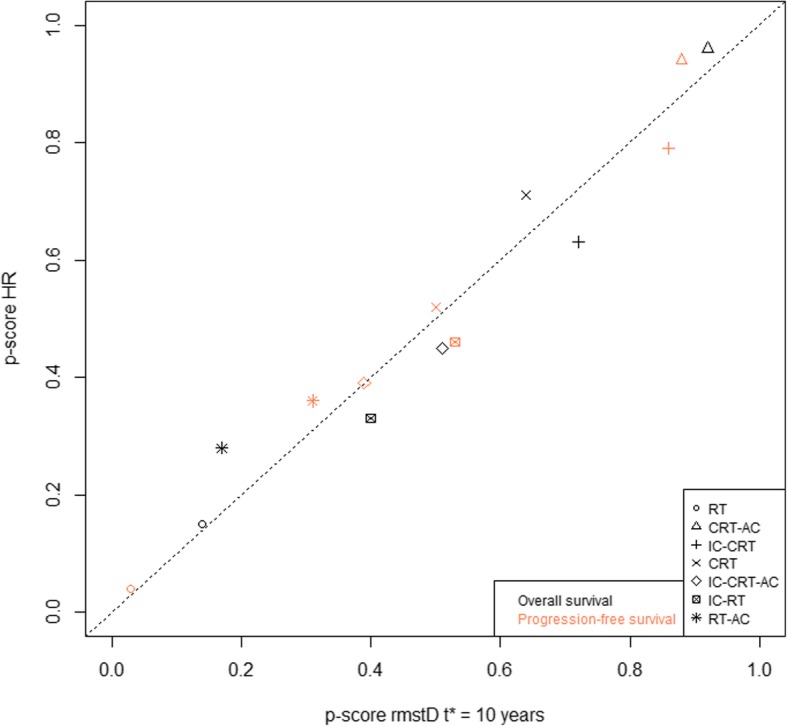
The three treatments that had the highest effect on OS with rmstD were CRT-AC, IC-CRT, and CRT (respective P scores of 92%, 72%, and 64%) compared to CRT-AC, CRT, and IC-CRT when using HR (respective P scores of 96%, 71%, and 63%). Of the 32 HR and rmstD analyzed, 5 had a different interpretation, 3 with a direction change (different direction of treatment effect) and 2 with a change in significance (same direction but a change in statistical significance). Results for secondary endpoints were overall in agreement.
The use of either HR or rmstD impacts the results of NMA. Given the sensitivity of HR to non-proportional hazards, this finding could have implications in terms of meta-analysis methodology.
本研究旨在应用受限平均生存时间差(rmstD)作为绝对结局指标进行网络荟萃分析,并将结果与最近由 MAC-NPC 协作组(Meta-Analysis of Chemotherapy [CT] in NPC)发表的关于化疗在鼻咽癌(NPC)中作用的个体患者数据(IPD)网络荟萃分析(NMA)中风险比(HR)得出的结果进行比较。
共纳入 20 项比较非转移性 NPC 中放疗(RT)联合或不联合化疗(CT)的临床试验(5144 例患者)。将治疗分为七类:单纯放疗(RT)、诱导 CT 后放疗(IC-RT)、放疗后辅助 CT(RT-AC)、IC-RT 后 AC、同期放化疗(CRT)、IC-RT 后 CRT(IC-CRT)和 CRT 后 AC(CRT-AC)。主要终点为总生存(OS);次要终点为无进展生存和局部区域控制。在每个试验中,rmstD 估计在 t*=10 年。应用随机效应频率主义 NMA 模型。采用 P 评分进行治疗排序。评估了异质性和不一致性。
与 HR 相比,用 rmstD 评估,OS 获益最高的三种治疗方法是 CRT-AC、IC-CRT 和 CRT(相应的 P 评分分别为 92%、72%和 64%),而 HR 的 P 评分分别为 96%、71%和 63%。在分析的 32 个 HR 和 rmstD 中,有 5 个结果不同,其中 3 个的治疗效果方向改变(不同的治疗效果方向),2 个的统计学意义改变(相同的治疗效果方向但统计学意义改变)。次要终点的结果总体一致。
HR 或 rmstD 的使用都会影响 NMA 的结果。鉴于 HR 对非比例风险的敏感性,这一发现可能对荟萃分析方法学产生影响。