Yim Kendrick, Bindayi Ahmet, McKay Rana, Mehrazin Reza, Raheem Omer A, Field Charles, Bloch Aaron, Wake Robert, Ryan Stephen, Patterson Anthony, Derweesh Ithaar H
Department of Urology, University of California at San Diego, La Jolla, CA, 92093, USA.
Department of Urology, University of Tennessee Health Sciences Center, Memphis, TN 38163, USA.
Cancers (Basel). 2019 Apr 15;11(4):536. doi: 10.3390/cancers11040536.
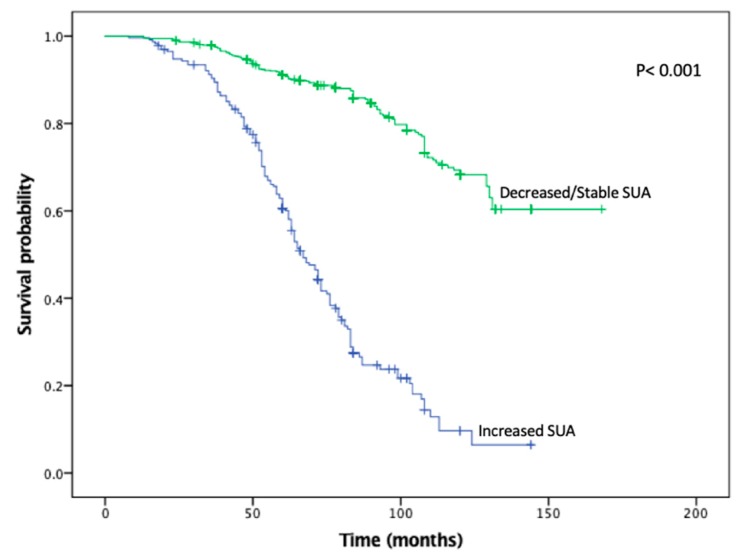
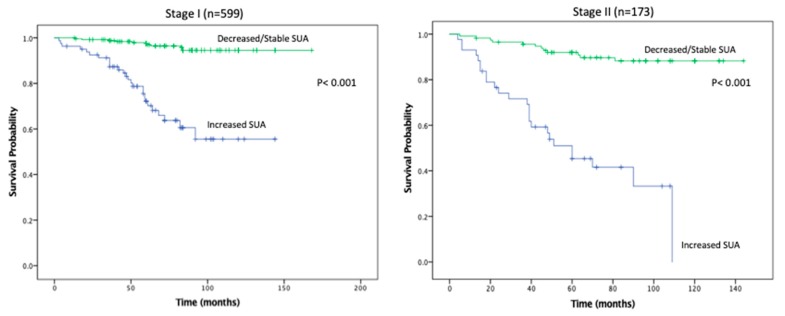
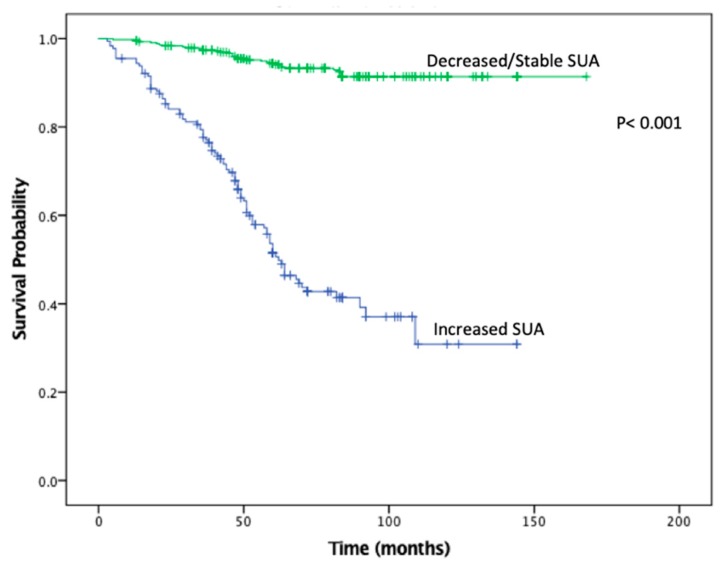
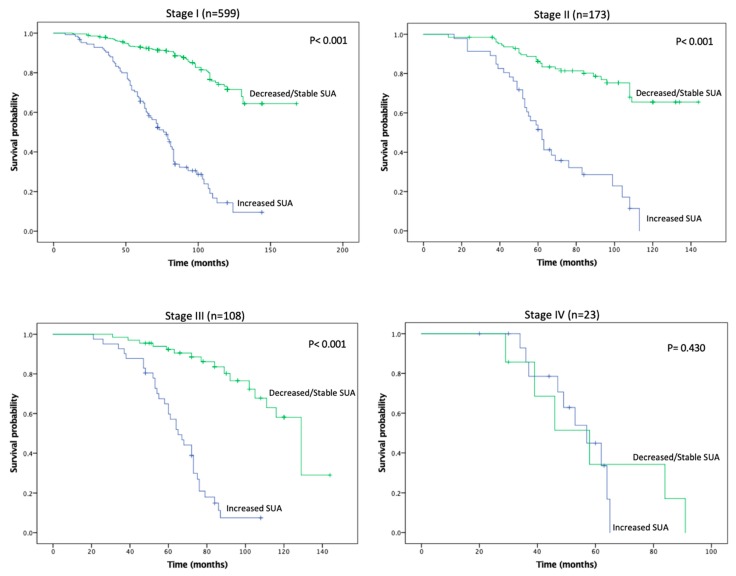
To investigate the association of serum uric acid (SUA) levels along with statin use in Renal Cell Carcinoma (RCC), as statins may be associated with improved outcomes in RCC and SUA elevation is associated with increased risk of chronic kidney disease (CKD). Retrospective study of patients undergoing surgery for RCC with preoperative/postoperative SUA levels between 8/2005-8/2018. Analysis was carried out between patients with increased postoperative SUA vs. patients with decreased/stable postoperative SUA. Kaplan-Meier analysis (KMA) calculated overall survival (OS) and recurrence free survival (RFS). Multivariable analysis (MVA) was performed to identify factors associated with increased SUA levels and all-cause mortality. The prognostic significance of variables for OS and RFS was analyzed by cox regression analysis. Decreased/stable SUA levels were noted in 675 (74.6%) and increased SUA levels were noted in 230 (25.4%). A higher proportion of patients with decreased/stable SUA levels took statins (27.9% vs. 18.3%, = 0.0039). KMA demonstrated improved 5- and 10-year OS (89% vs. 47% and 65% vs. 9%, < 0.001) and RFS (94% vs. 45% and 93% vs. 34%, < 0.001), favoring patients with decreased/stable SUA levels. MVA revealed that statin use (Odds ratio (OR) 0.106, < 0.001), dyslipidemia (OR 2.661, = 0.004), stage III and IV disease compared to stage I (OR 1.887, = 0.015 and 10.779, < 0.001, respectively), and postoperative de novo CKD stage III (OR 5.952, < 0.001) were predictors for increased postoperative SUA levels. MVA for all-cause mortality showed that increasing BMI (OR 1.085, = 0.002), increasing ASA score (OR 1.578, = 0.014), increased SUA levels (OR 4.698, < 0.001), stage IV disease compared to stage I (OR 7.702, < 0.001), radical nephrectomy (RN) compared to partial nephrectomy (PN) (OR 1.620, = 0.019), and de novo CKD stage III (OR 7.068, < 0.001) were significant factors. Cox proportional hazard analysis for OS revealed that increasing age (HR 1.017, = 0.004), increasing BMI (Hazard Ratio (HR) 1.099, < 0.001), increasing SUA (HR 4.708, < 0.001), stage III and IV compared to stage I (HR 1.537, = 0.013 and 3.299, < 0.001), RN vs. PN (HR 1.497, = 0.029), and de novo CKD stage III (HR 1.684, < 0.001) were significant factors. Cox proportional hazard analysis for RFS demonstrated that increasing ASA score (HR 1.239, < 0.001, increasing SUA (HR 9.782, < 0.001), and stage II, III, and IV disease compared to stage I (HR 2.497, < 0.001 and 3.195, < 0.001 and 6.911, < 0.001) were significant factors. : Increasing SUA was associated with poorer outcomes. Decreased SUA levels were associated with statin intake and lower stage disease as well as lack of progression to CKD and anemia. Further investigation is requisite.
为研究肾细胞癌(RCC)患者血清尿酸(SUA)水平与他汀类药物使用之间的关联,因为他汀类药物可能与RCC患者预后改善相关,且SUA升高与慢性肾脏病(CKD)风险增加相关。对2005年8月至2018年8月期间接受RCC手术且术前/术后有SUA水平记录的患者进行回顾性研究。对术后SUA升高的患者与术后SUA降低/稳定的患者进行分析。采用Kaplan-Meier分析(KMA)计算总生存期(OS)和无复发生存期(RFS)。进行多变量分析(MVA)以确定与SUA水平升高和全因死亡率相关的因素。通过Cox回归分析评估各变量对OS和RFS的预后意义。675例(74.6%)患者SUA水平降低/稳定,230例(25.4%)患者SUA水平升高。SUA水平降低/稳定的患者中服用他汀类药物的比例更高(27.9%对18.3%,P = 0.0039)。KMA显示,5年和10年OS(89%对47%以及65%对9%,P < 0.001)和RFS(94%对45%以及93%对34%,P < 0.001)均有所改善,SUA水平降低/稳定的患者预后更佳。MVA显示,使用他汀类药物(比值比(OR)0.106,P < 0.001)、血脂异常(OR 2.661,P = 0.004)、与I期相比的III期和IV期疾病(OR分别为1.887,P = 0.015和10.779,P < 0.001)以及术后新发CKD III期(OR 5.95