Centre for Health Policy, Melbourne School of Population and Global Health, The University of Melbourne, Level 4, 207 Bouverie St, Carlton, VIC, 3010, Australia.
Centre for Health Economics, Monash Business School, Monash University, Building H, Level 5, Caulfield, VIC, 3145, Australia.
Int J Equity Health. 2019 Apr 16;18(1):57. doi: 10.1186/s12939-019-0955-9.
Income-related inequality measures such as the concentration index are often used to describe the unequal distribution of health, health care access, or expenditure in a single measure. This study demonstrates the use of such measures to evaluate the distributional impact of changes in health insurance coverage. We use the example of Medicare Part D in the United States, which increased access to prescription medications for Medicare beneficiaries from 2006.
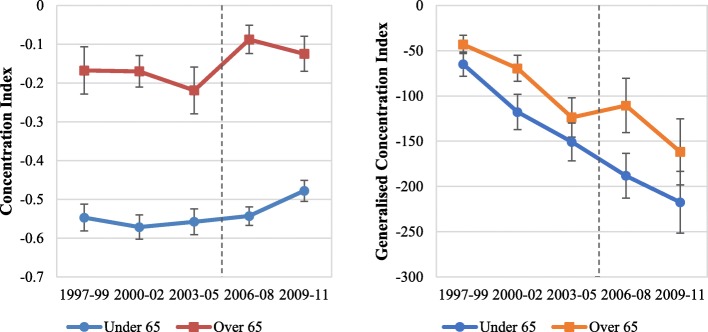
Using pooled cross-sectional samples from the Medical Expenditure Panel Survey for 1997-2011, we estimated income-related inequality in drug expenditures over time using the concentration and generalised concentration indices. A difference-in-differences analysis investigated the change in inequality in drug expenditures, as measured using the concentration index and generalised concentration index, between the elderly (over 65 years) and near-elderly (54-63 years) pre- and post-implementation of Medicare Part D.
Medicare Part D increased public drug expenditure while out-of-pocket and private spending fell. Public drug expenditures favoured the poor during all study periods, but the degree of pro-poorness declined in the years immediately following the implementation of Part D, with the poor gaining less than the rich in both relative and absolute terms. Part D also appeared to result in a fall in the pro-richness of private insurance drug expenditure in absolute terms but have minimal distributional impact on out-of-pocket expenditure. These effects appeared to be short lived, with a return to the prevailing trends in both concentration and generalised concentration indices several years following the start of Part D.
The implementation of Medicare Part D significantly reduced the degree of pro-poorness in public drug expenditure. The poor gained less of the increased public drug expenditure than the rich in both relative and absolute terms. This study demonstrates how income-related inequality measures can be used to estimate the impact of health system changes on inequalities in health expenditure and provides a guide for future evaluations.
收入相关的不平等指标,如集中指数,通常用于单一指标描述健康、医疗保健可及性或支出的不平等分布。本研究展示了如何使用这些指标来评估医疗保险覆盖范围变化的分配影响。我们以美国的医疗保险处方药部分(Medicare Part D)为例,该部分从 2006 年开始增加了医疗保险受益人的处方药可及性。
使用 1997 年至 2011 年期间医疗支出面板调查的汇总横截面样本,我们使用集中指数和广义集中指数,随时间推移估计药物支出的收入相关不平等情况。差异中的差异分析调查了在实施医疗保险处方药部分前后(65 岁以上和 54-63 岁),药物支出不平等程度(使用集中指数和广义集中指数衡量)的变化。
医疗保险处方药部分增加了公共药物支出,而自付和私人支出下降。在所有研究期间,公共药物支出都有利于穷人,但在实施处方药部分后的几年里,亲贫程度下降,相对和绝对而言,穷人的获益都低于富人。处方药部分似乎也导致私人保险药物支出的亲富程度在绝对值上下降,但对自付支出的分配影响微不足道。这些影响似乎是短暂的,在实施处方药部分几年后,集中和广义集中指数的流行趋势又恢复了。
医疗保险处方药部分的实施显著降低了公共药物支出的亲贫程度。相对和绝对而言,穷人从增加的公共药物支出中获益都低于富人。本研究展示了如何使用收入相关的不平等指标来估计卫生系统变化对健康支出不平等的影响,并为未来的评估提供了指导。