Department of Radiation Oncology, Klinikum rechts der Isar, Technical University Munich, Ismaninger Str. 22, 81675, Munich, Germany.
German Cancer Consortium (DKTK), Partner Site Munich, Munich, Germany.
Radiat Oncol. 2019 Apr 16;14(1):66. doi: 10.1186/s13014-019-1270-8.
Multimodal treatment with neoadjuvant chemoradiation followed by surgery (nCRT + S) is the treatment of choice for patients with locally advanced or node-positive esophageal squamous cell carcinoma (E-SCC). Those who are unsuitable or who decline surgery can be treated with definitive chemoradiation (dCRT). This study compares the oncologic outcome of nCRT + S and dCRT in E-SCC patients.
Between 2011 and 2017, 95 patients with E-SCC were scheduled for dCRT or nCRT+ S with IMRT at our department. Patients undergoing dCRT received at least 50 Gy and those undergoing nCRT + S received at least 41.4 Gy. All patients received simultaneous chemotherapy with either carboplatin and paclitaxel or cisplatin and 5-fluoruracil. We retrospectively compared baseline characteristics and oncologic outcome including overall survival (OS), progression-free survival (PFS) and site of failure between both treatment groups.
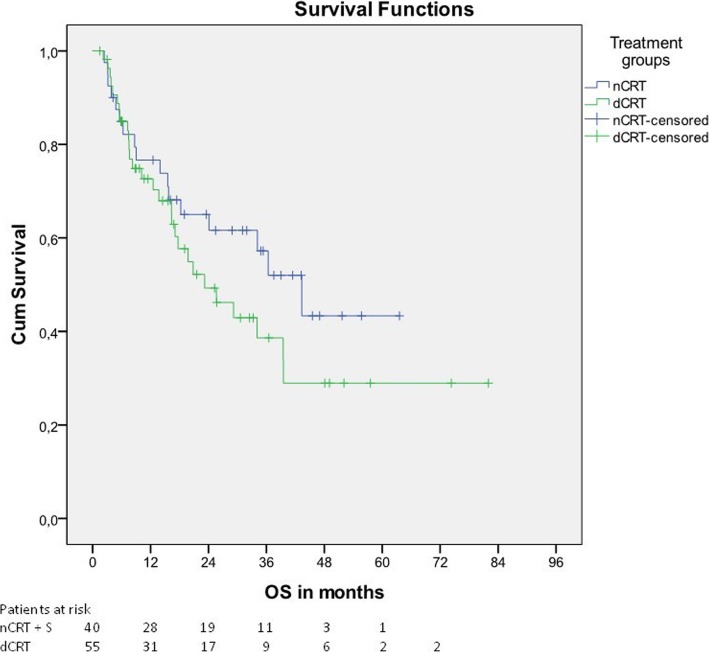
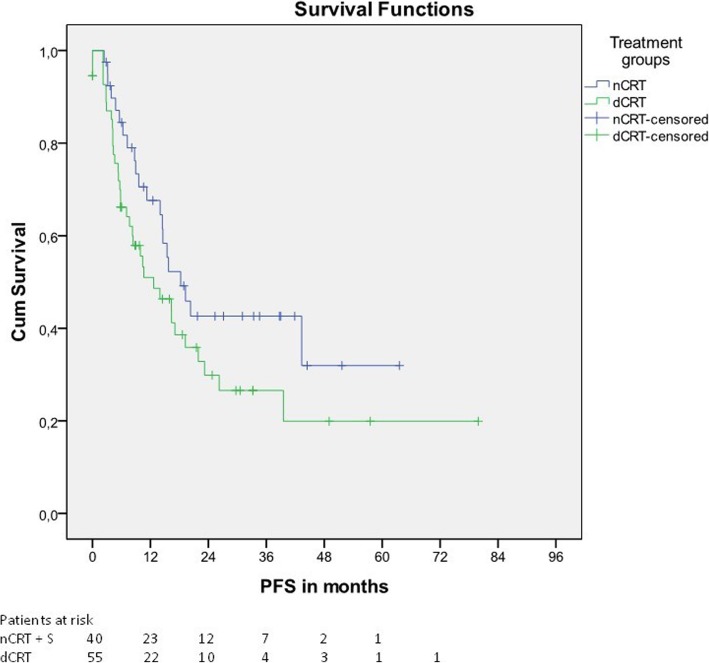
Patients undergoing dCRT were less likely to have clinically suspected lymph node metastases (85% vs. 100%, p = 0.019) than patients undergoing nCRT + S and had more proximally located tumors (median distance from dental arch to cranial tumor border 20 cm vs. 26 cm, p < 0.001). After a median follow up of 25.6 months for surviving patients, no significant differences for OS and PFS were noticed comparing nCRT + S and dCRT. However, the rate of local tumor recurrence was significantly higher in patients treated with dCRT than in those treated with nCRT + S (38% vs. 10%, p = 0.002). Within a multivariate Cox regression model, age, tumor location, and tumor grading were the only independent parameters affecting OS and PFS. In addition to that, proximal tumor location was the only parameter independently associated with an increased risk for local treatment failure.
In E-SCC patients treated with either dCRT or nCRT + S, a higher rate of local tumor recurrence was seen in patients treated with dCRT than in patients treated with nCRT + S. There was at least a trend towards an improved OS and PFS in patients undergoing nCRT + S. However, this should be interpreted with caution, because proximal tumor location was the only parameter independently affecting the risk of local tumor recurrence.
新辅助放化疗后手术(nCRT+S)联合治疗是局部晚期或淋巴结阳性食管鳞癌(E-SCC)患者的首选治疗方法。不适合或拒绝手术的患者可采用根治性放化疗(dCRT)。本研究比较了 nCRT+S 和 dCRT 在 E-SCC 患者中的肿瘤学结局。
2011 年至 2017 年,我院 95 例 E-SCC 患者行 dCRT 或 nCRT+S 治疗,均采用调强放疗。dCRT 组患者接受至少 50Gy,nCRT+S 组患者接受至少 41.4Gy。所有患者均接受顺铂联合紫杉醇或顺铂联合氟尿嘧啶同步化疗。我们回顾性比较了两组患者的基线特征和肿瘤学结局,包括总生存期(OS)、无进展生存期(PFS)和失败部位。
与 nCRT+S 组患者(100%)相比,行 dCRT 的患者临床疑似淋巴结转移的可能性更低(85%,p=0.019),肿瘤位置更靠近近端(从齿弓到颅肿瘤边界的中位距离为 20cm 比 26cm,p<0.001)。对存活患者进行中位随访 25.6 个月后,nCRT+S 和 dCRT 两组间 OS 和 PFS 无显著差异。然而,dCRT 组局部肿瘤复发率明显高于 nCRT+S 组(38%比 10%,p=0.002)。在多因素 Cox 回归模型中,年龄、肿瘤位置和肿瘤分级是影响 OS 和 PFS 的唯一独立参数。此外,近端肿瘤位置是与局部治疗失败风险增加相关的唯一参数。
在接受 dCRT 或 nCRT+S 治疗的 E-SCC 患者中,dCRT 组患者局部肿瘤复发率高于 nCRT+S 组。nCRT+S 组患者的 OS 和 PFS 至少有改善趋势。然而,这应谨慎解读,因为近端肿瘤位置是唯一独立影响局部肿瘤复发风险的参数。