UCLH-UCL Centre for Medicines Optimisation Research and Education, Pharmacy Department, University College London Hospitals NHS Foundation Trust, 235 Euston Road, London, NW1 2BU, UK.
UCLH-UCL Centre for Medicines Optimisation Research and Education, UCL School of Pharmacy, 29-39, Brunswick Square, London, WC1N 1AX, UK.
Support Care Cancer. 2019 Jul;27(7):2413-2424. doi: 10.1007/s00520-019-04773-6. Epub 2019 Apr 16.
Neutropenia is associated with an increased risk of mortality and hospitalisation. Strategies, including the prescribing of colony-stimulating growth factors (CSFs), are adopted when a high risk (> 20%) of neutropenic complications are seen in the clinical trial setting. With a diverse treatment population that may differ from the patient groups recruited to studies, appropriate prescribing decisions by clinicians are essential. At present, results are conflicting from studies evaluating the risks of certain patient attributes on neutropenic events; we aimed to aggregate these associations to guide future management.
A systematic review with a meta-analysis was conducted using the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement. Studies were identified through a literature search using MEDLINE, EMBASE and Cumulative Index to Nursing and Allied Health Literature (CINAHL) databases from inception to December 1, 2017. Studies were included into a meta-analysis if they adjusted for confounders; analyses were conducted in STATA v 15.1 SE.
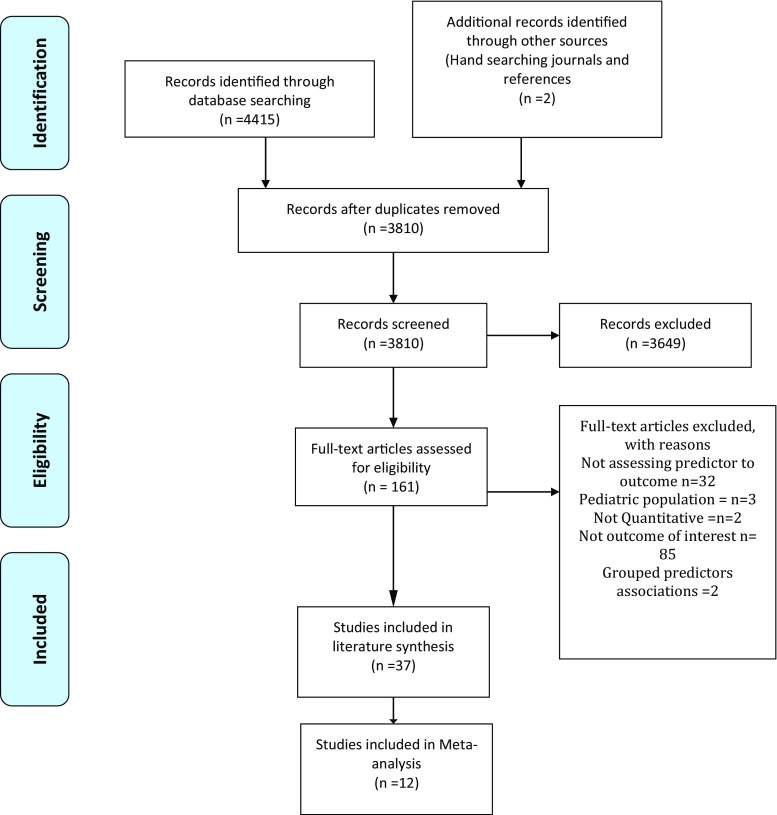
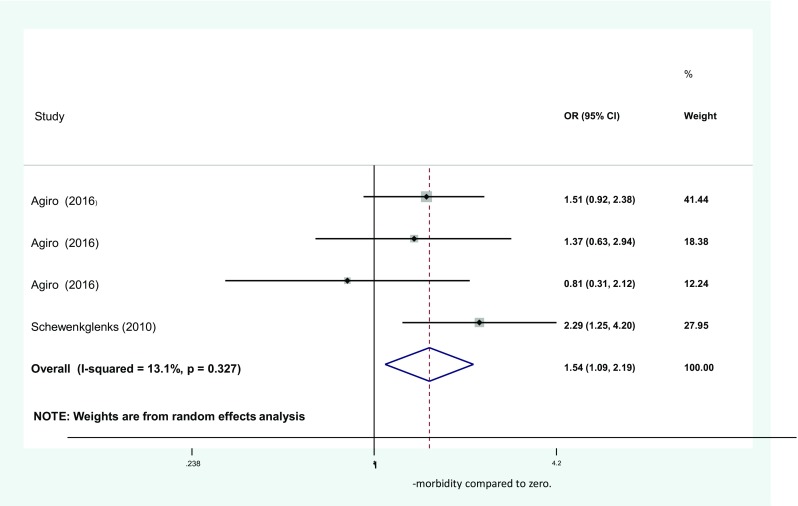
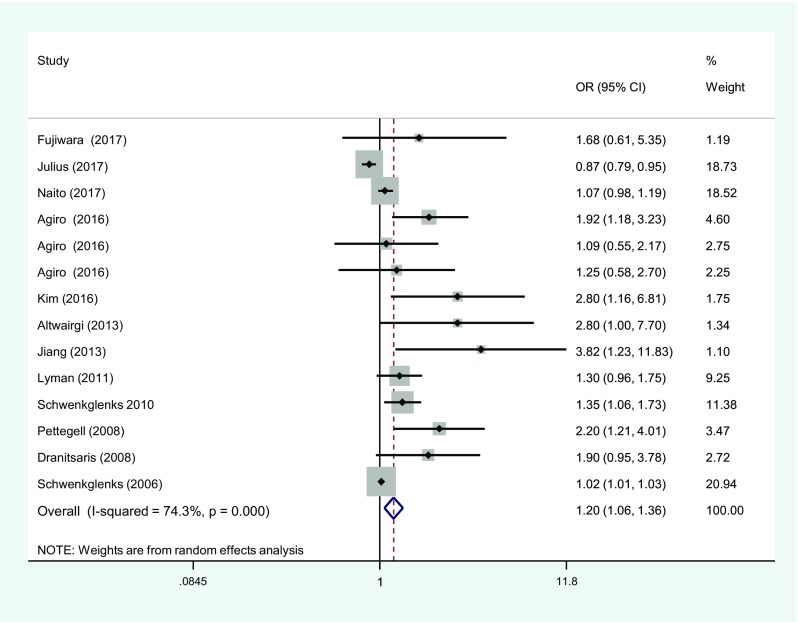
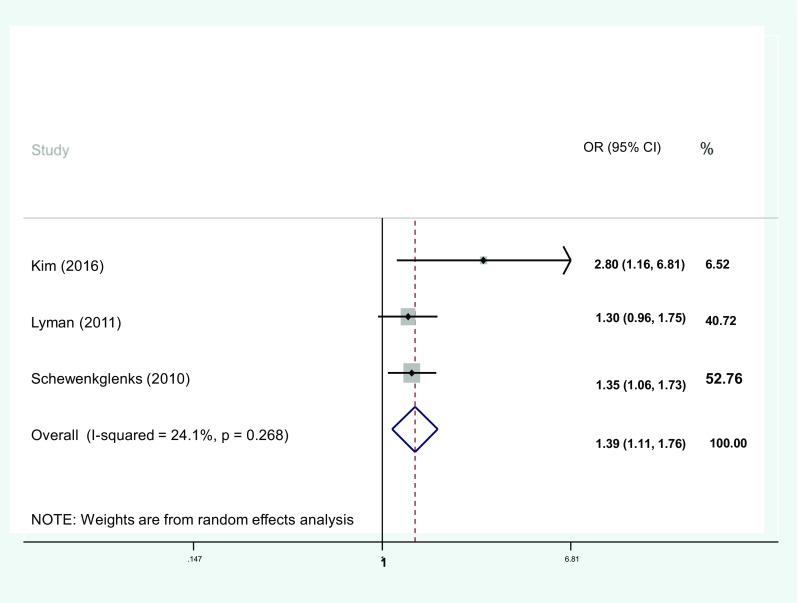
A total of 4415 articles were retrieved by the search with 37 meeting the inclusion criteria and 12 eligible for meta-analysis. Meta-analysis was conducted for increasing age and yielded a pooled odds ratio of 1.39 (1.11, 1.76, I = 24.1%), in our subgroup analysis of 4814 patients. Odds ratios for studies were pooled that reported associations for one co-morbidity compared to none and resulted in an overall odds of 1.54 (CI 1.09-2.09, I = 13.1%), including 9189 patients in total.
Results can enhance current guidance in prescribing primary prophylaxis for treatments that either fall marginally under the internationally recognised 20% neutropenia risk.
中性粒细胞减少与死亡率和住院风险增加相关。在临床试验中,如果观察到发生中性粒细胞减少并发症的风险较高(>20%),则会采用包括集落刺激因子(CSF)在内的治疗策略。由于治疗人群可能与研究中招募的患者群体不同,因此临床医生的适当处方决策至关重要。目前,评估某些患者特征对中性粒细胞减少事件风险的研究结果存在矛盾;我们旨在汇总这些关联以指导未来的管理。
采用系统评价和荟萃分析,使用系统评价和荟萃分析首选报告项目(PRISMA)声明进行。通过 MEDLINE、EMBASE 和 Cumulative Index to Nursing and Allied Health Literature(CINAHL)数据库进行文献检索,从开始到 2017 年 12 月 1 日,检索到 4415 篇文章,其中 37 篇符合纳入标准,12 篇符合荟萃分析条件。如果研究调整了混杂因素,则进行荟萃分析;在 STATA v 15.1 SE 中进行分析。
通过搜索共检索到 4415 篇文章,其中 37 篇符合纳入标准,12 篇符合荟萃分析条件。在我们对 4814 名患者的亚组分析中,对年龄增长进行荟萃分析,得出合并优势比为 1.39(1.11,1.76,I=24.1%)。对报告与无合并症相比有一种合并症的研究进行汇总,得出总体优势比为 1.54(CI 1.09-2.09,I=13.1%),总共包括 9189 名患者。
这些结果可以增强目前在处方主要预防治疗方面的指导,这些治疗方案要么略低于国际公认的 20%中性粒细胞减少风险。