Department of Rheumatology and Clinical Immunology, Peking University First Hospital, No. 8 Xishiku Street, West District, Beijing, 100034, China.
Arthritis Res Ther. 2019 Apr 17;21(1):100. doi: 10.1186/s13075-019-1892-0.
Ultrasound (US) is sensitive for detecting joint and tendon inflammation in patients with rheumatoid arthritis (RA). So far, which grade of abnormalities on US corresponds to clinical manifestations is unclear. This study aimed to investigate the agreement between US-detected joint inflammation and clinical signs (joint swelling and tenderness).
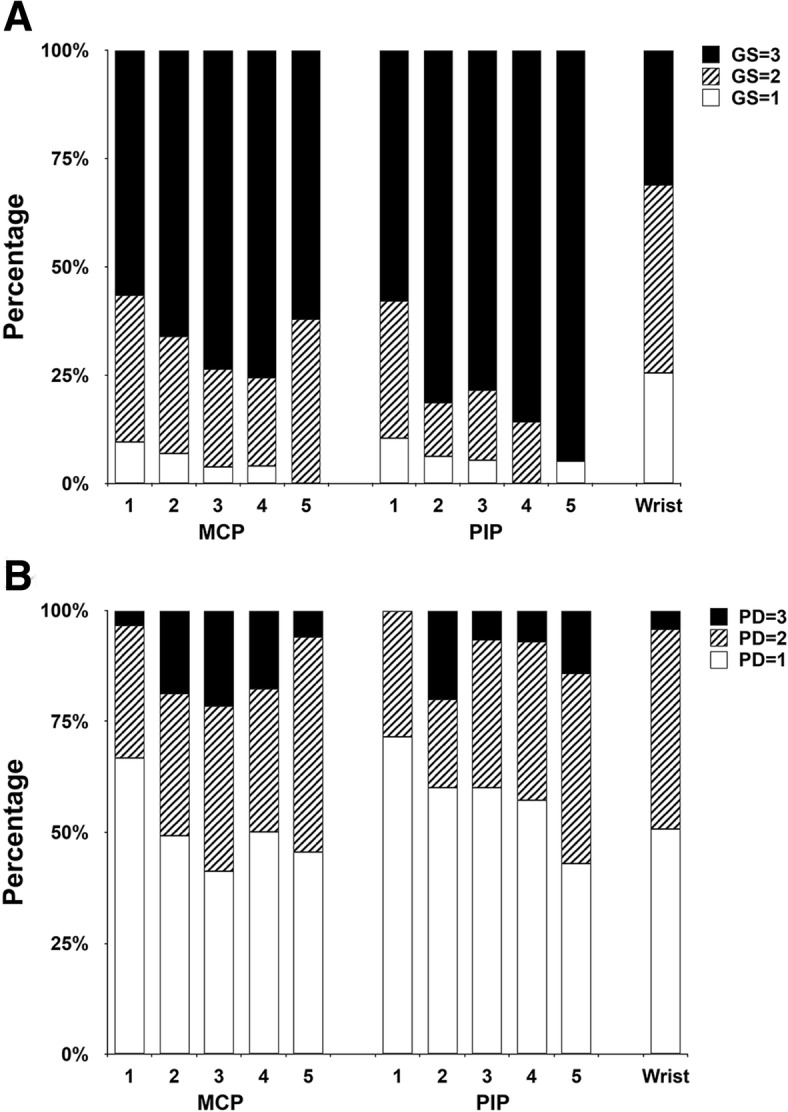
In this cross-sectional study, 22 joints of the wrists and hands were, respectively, evaluated by physical examination (PE) and ultrasound in RA patients. Gray scale (GS) and power Doppler (PD) of synovitis, detected by ultrasound, were graded by semi-quantitative scoring systems (0-3). Tenosynovitis and peritendinitis were assessed qualitatively (0/1).
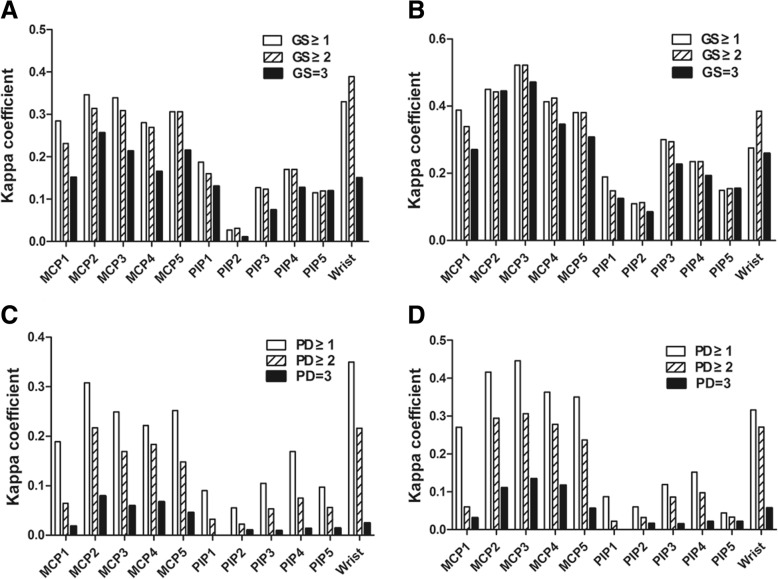
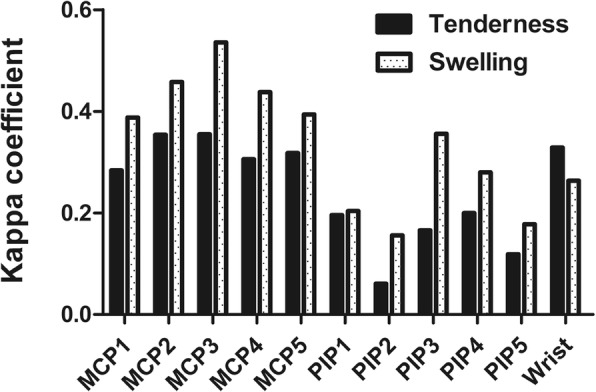
A total of 258 consecutive RA patients were included, with median disease duration of 57 months and mean Disease Activity Score based on 28 joints (DAS28)-ESR/DAS28-CRP of 4.47/3.99. In a total of 5676 joints assessed, the overall concordance rate between positive clinical signs and ultrasound-determined joint inflammation was fair (κ = 0.365, p < 0.01). In wrists, joint tenderness showed higher κ coefficient (κ = 0.329, p < 0.01) with ultrasound-determined joint inflammation than swelling (κ = 0.263, p < 0.01); however, swelling showed higher κ coefficient (κ = 0.156-0.536, p < 0.01) with ultrasound-determined joint inflammation than tenderness (κ = 0.061-0.355, p < 0.01) in metacarpophalangeal (MCP) and proximal interphalangeal (PIP) joints. Synovitis had consistently higher agreement with tenderness and swelling than tenosynovitis/peritendinitis. Tenderness and swelling had the highest κ coefficient with GS ≥ 1 synovial hyperplasia in most MCP and PIP joints, while with GS ≥ 2 synovial hyperplasia in wrists. For all 22 joints, PD ≥ 1 synovitis had the highest κ coefficient with clinical tenderness and swelling.
Synovitis had better agreement with clinical signs than tenosynovitis/peritendinitis. Joint swelling showed better agreement with US-determined inflammation than tenderness for MCP and PIP joints, while the opposite for wrists. Both tenderness and swelling are more likely to correspond to GS ≥ 2 for wrists, GS ≥ 1 for MCP and PIP joints, and PD ≥ 1 for any joint.
超声(US)对于检测类风湿关节炎(RA)患者的关节和肌腱炎症非常敏感。到目前为止,US 检测到的异常程度与临床表现相对应还不清楚。本研究旨在探讨 US 检测到的关节炎症与临床体征(关节肿胀和压痛)之间的一致性。
在这项横断面研究中,分别通过体格检查(PE)和超声对 22 个腕关节和手部关节进行评估。通过半定量评分系统(0-3 分)对超声检测到的滑膜炎的灰度(GS)和功率多普勒(PD)进行分级。肌腱滑膜炎和肌腱周围炎通过定性评估(0/1)。
共纳入 258 例连续的 RA 患者,中位病程为 57 个月,基于 28 个关节的疾病活动评分(DAS28)-红细胞沉降率/基于 28 个关节的 DAS28-CRP 分别为 4.47/3.99。在评估的 5676 个关节中,阳性临床体征与超声确定的关节炎症之间的总体一致性率为中度(κ=0.365,p<0.01)。在腕关节中,与超声确定的关节炎症相比,关节压痛的 κ 系数更高(κ=0.329,p<0.01),而肿胀的 κ 系数较低(κ=0.263,p<0.01);然而,与超声确定的关节炎症相比,肿胀在掌指关节(MCP)和近端指间关节(PIP)中具有更高的 κ 系数(κ=0.156-0.536,p<0.01),而压痛的 κ 系数较低(κ=0.061-0.355,p<0.01)。滑膜炎与压痛和肿胀的一致性始终高于肌腱滑膜炎/肌腱周围炎。在大多数 MCP 和 PIP 关节中,GS≥1 滑膜增生与压痛和肿胀的 κ 系数最高,而在腕关节中则为 GS≥2 滑膜增生。对于所有 22 个关节,PD≥1 滑膜炎与临床压痛和肿胀的 κ 系数最高。
滑膜炎与临床体征的一致性优于肌腱滑膜炎/肌腱周围炎。与 MCP 和 PIP 关节相比,关节肿胀与 US 确定的炎症比压痛更一致,而在腕关节中则相反。对于腕关节,GS≥2,MCP 和 PIP 关节 GS≥1,任何关节 PD≥1,压痛和肿胀更有可能对应。