Ahmad Raheelah, Zhu Nina Jiayue, Lebcir Reda Mohamed, Atun Rifat
NIHR Health Protection Research Unit in Healthcare Associated Infection and Antimicrobial Resistance, Imperial College London, London, UK.
Institute of Business Administration, Karachi, Karachi, Pakistan.
BMJ Glob Health. 2019 Mar 30;4(2):e001242. doi: 10.1136/bmjgh-2018-001242. eCollection 2019.
Limited studies have explored how health-seeking behaviour during pregnancy through to delivery affect neonatal outcomes. We modelled health-seeking behaviour across urban and rural settings in Pakistan, where poor neonatal outcomes persist with wide disparities.
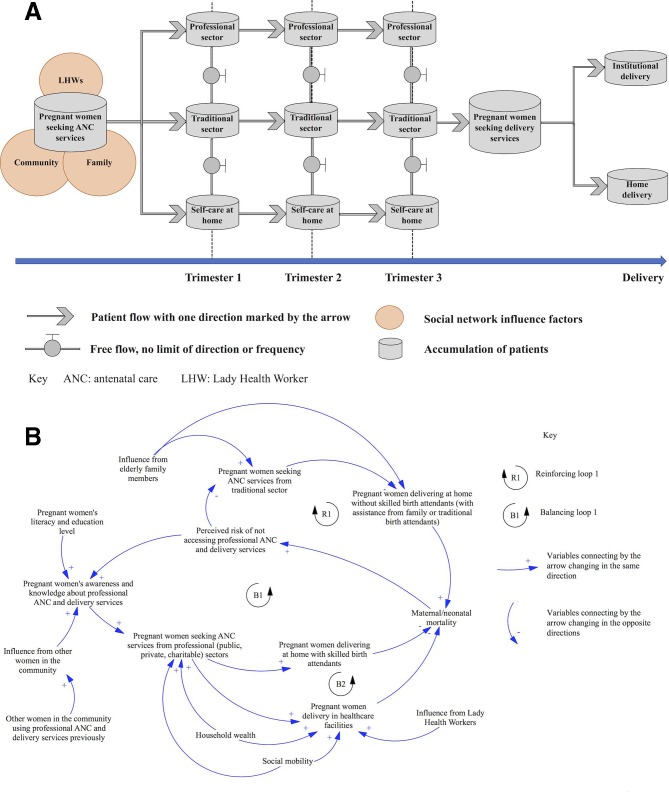
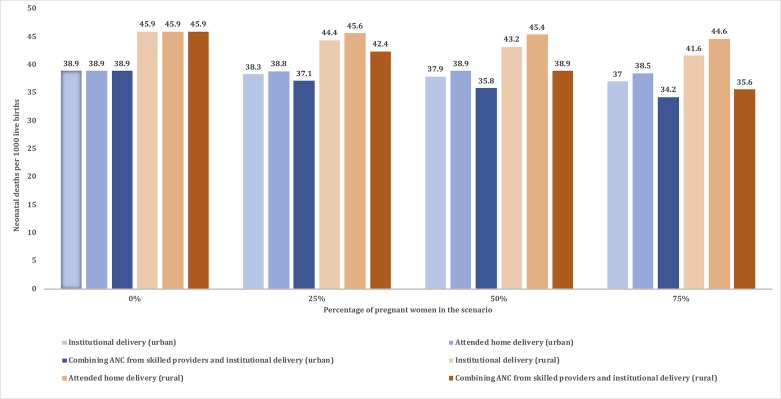
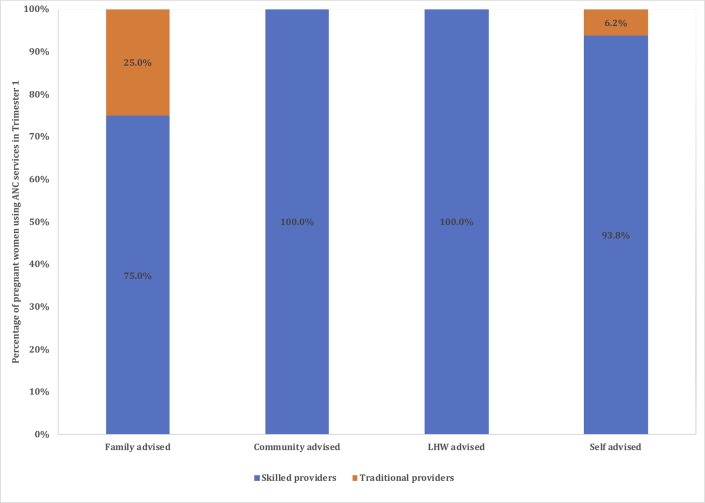
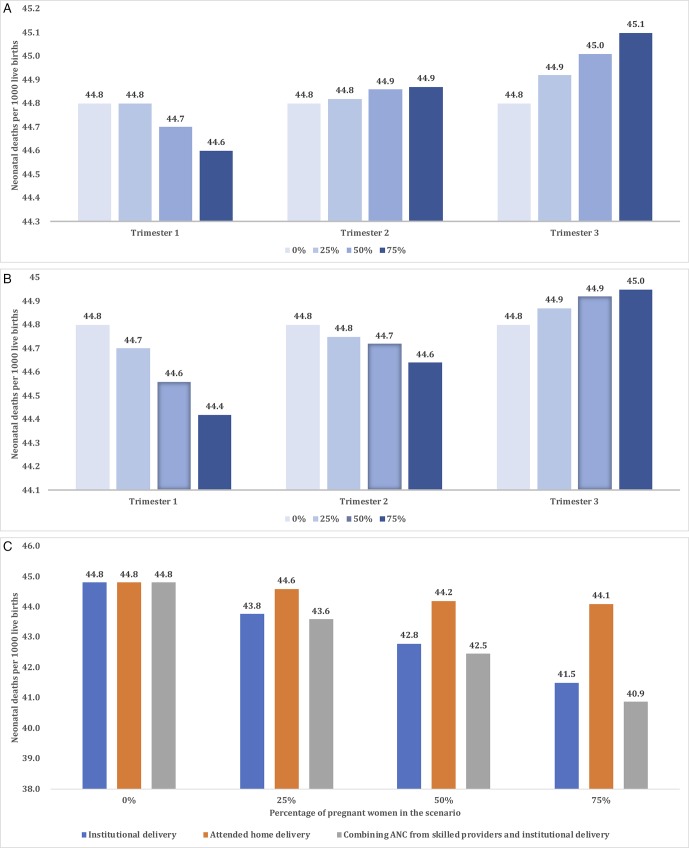
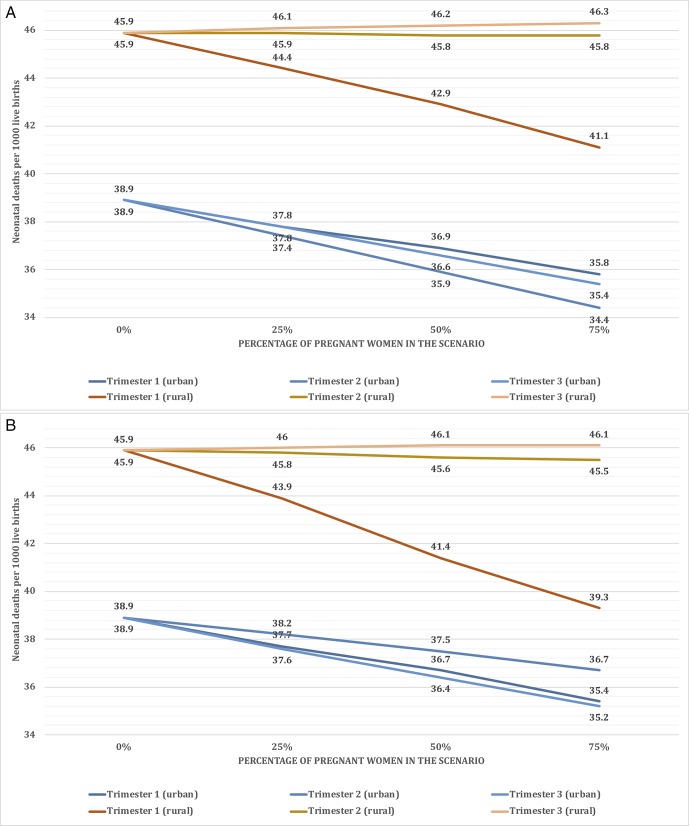
A system dynamics model was developed and parameterised. Following validation tests, the model was used to determine neonatal mortality for pregnant women considering their decisions to access, refuse and switch antenatal care services in four provider sectors: public, private, traditional and charitable. Four health-seeking scenarios were tested across different pregnancy trimesters. Health-seeking behaviour in different subgroups by geographical locations and social network effect was modelled. The largest reduction in neonatal mortality was achieved with antenatal care provided by skilled providers in public, private or charitable sectors, combined with the use of institutional delivery. Women's social networks had strong influences on to seek care. Interventions by Lady Health Workers had a minimal impact on health-seeking behaviour and neonatal outcomes after trimester 1. Optimal benefits were achieved for urban women when antenatal care was accessed within trimester 2, but for rural women within trimester 1. Antenatal care access delayed to trimester 3 had no protective impact on neonatal mortality.
System dynamics modelling enables capturing the complexity of health-seeking behaviours and impact on outcomes, informing intervention design, implementation of targeted policies and uptake of services specific to urban/rural settings considering structural enablers/barriers to access, cultural contexts and strong social network influences.
仅有有限的研究探讨了从孕期到分娩期间的就医行为如何影响新生儿结局。我们对巴基斯坦城乡地区的就医行为进行了建模,该国新生儿结局较差且差异巨大。
开发并参数化了一个系统动力学模型。经过验证测试后,该模型用于确定孕妇的新生儿死亡率,同时考虑她们在四个医疗服务提供部门(公立、私立、传统和慈善部门)中选择、拒绝和更换产前护理服务的决定。在不同孕期测试了四种就医情景。对不同地理位置和社会网络效应的亚组中的就医行为进行了建模。由公立、私立或慈善部门的专业医护人员提供产前护理,并结合使用机构分娩,可使新生儿死亡率最大程度降低。女性的社会网络对其就医行为有很大影响。孕期1之后,女性卫生工作者的干预对就医行为和新生儿结局的影响极小。对于城市女性,在孕期2内接受产前护理可实现最佳效果,而对于农村女性,则在孕期1内接受产前护理可实现最佳效果。延迟到孕期3才获得产前护理对新生儿死亡率没有保护作用。
系统动力学建模能够把握就医行为的复杂性及其对结局的影响,为干预设计、针对性政策的实施以及考虑到获取服务的结构性促进因素/障碍、文化背景和强大社会网络影响的城乡特定环境下服务的采用提供信息。