Department of Surgery, University of Hawaii, Honolulu, HI, USA.
Cancer Center, University of Hawaii, Honolulu, HI, USA.
Clin Mol Hepatol. 2019 Sep;25(3):305-316. doi: 10.3350/cmh.2019.0004. Epub 2019 Apr 19.
BACKGROUND/AIMS: Inflammation-based scores, such as the neutrophil-to-lymphocyte ratio (NLR), have been associated with prognosis in hepatocellular carcinoma (HCC); but variable cut-off values and potential lack of specificity have limited the utility of NLR. This study evaluates NLR in a large cohort of HCC patients.
We retrospectively reviewed 789 HCC cases (1993-2017) for demographics, tumor characteristics, treatment, and survival. NLR was stratified into NLR ≥1.5 and NLR ≥3 and analyzed for correlation with American Joint Committee on Cancer (AJCC) and Barcelona Clinic Liver Cancer (BCLC) stages. In 235 patients who underwent liver resection, survival and recurrence were evaluated by NLR.
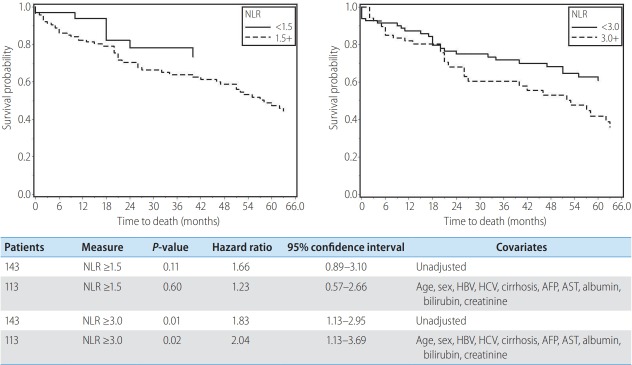
In 789 HCC cases, mean NLR was increased with advanced AJCC and BCLC stages. Hepatitis C patients were less likely to have NLR ≥1.5 and ≥3. Non-alcoholic steatohepatitis patients were more likely to have NLR ≥3. Patients with tumor size >5 cm, rupture, or macrovascular invasion were more likely to have NLR ≥3. In patients treated with resection, NLR ≥3 predicted early recurrence (odds ratio [OR] 4.14, P<0.01) and overall recurrence (OR 4.05, P<0.01). Mean NLR was 4.30 in those with recurrence and 2.75 in those without recurrence. Patients with NLR ≥3 showed significantly worse survival compared to those with NLR <3 (P<0.01 by log-rank test).
Elevated NLR is associated with advanced cancer stage and aggressive tumor characteristics, such as large size, rupture, and invasion. NLR ≥3 was associated with early and overall recurrence after resection but varied with etiology. NLR may be a useful biomarker in predicting recurrence for HCC patients undergoing curative resection, but further studies are required to elucidate the effect of disease etiology.
背景/目的:基于炎症的评分,如中性粒细胞与淋巴细胞比值(NLR),与肝细胞癌(HCC)的预后相关;但 NLR 的截止值不同且缺乏特异性,限制了其应用。本研究评估了大量 HCC 患者的 NLR。
我们回顾性分析了 789 例 HCC 病例(1993-2017 年)的人口统计学、肿瘤特征、治疗和生存情况。将 NLR 分为 NLR≥1.5 和 NLR≥3,并分析与美国癌症联合委员会(AJCC)和巴塞罗那临床肝癌(BCLC)分期的相关性。在 235 例接受肝切除术的患者中,通过 NLR 评估生存和复发情况。
在 789 例 HCC 病例中,随着 AJCC 和 BCLC 分期的进展,NLR 均值逐渐增加。丙型肝炎患者 NLR≥1.5 和≥3 的可能性较小。非酒精性脂肪性肝炎患者 NLR≥3 的可能性更大。肿瘤直径>5cm、破裂或大血管侵犯的患者 NLR≥3 的可能性更大。在接受切除术治疗的患者中,NLR≥3 预测早期复发(优势比[OR]4.14,P<0.01)和总体复发(OR 4.05,P<0.01)。复发患者的 NLR 均值为 4.30,无复发患者的 NLR 均值为 2.75。NLR≥3 的患者的生存明显差于 NLR<3 的患者(对数秩检验,P<0.01)。
升高的 NLR 与晚期癌症分期和侵袭性肿瘤特征相关,如肿瘤较大、破裂和侵犯。NLR≥3 与肝切除术后早期和总体复发相关,但因病因而异。NLR 可能是预测 HCC 患者根治性切除术后复发的有用生物标志物,但需要进一步研究来阐明疾病病因的影响。