Emerg Infect Dis. 2019 May;25(5):856-864. doi: 10.3201/eid2505.181141.
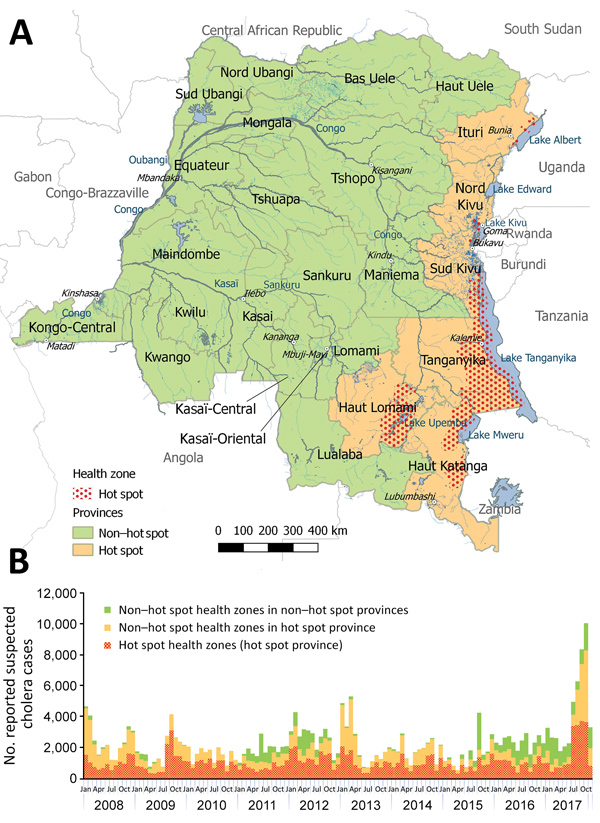
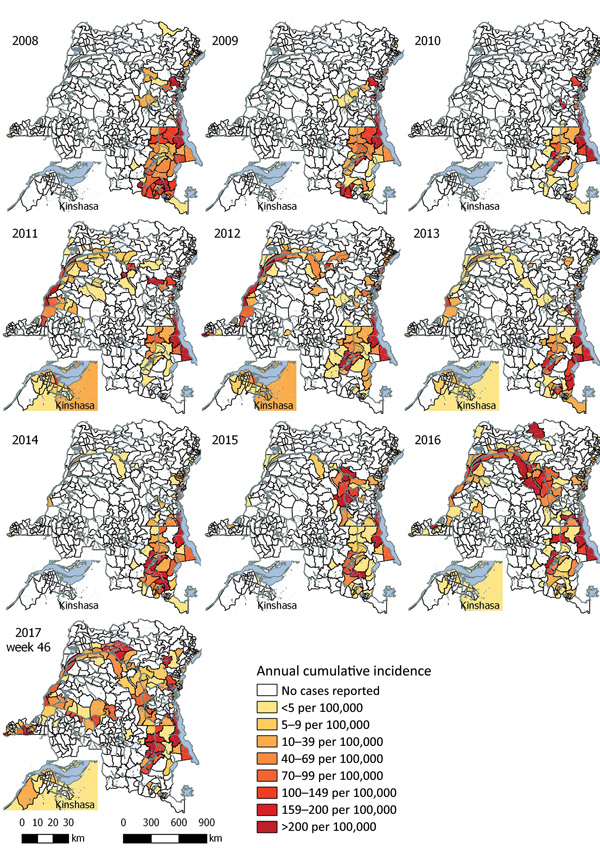
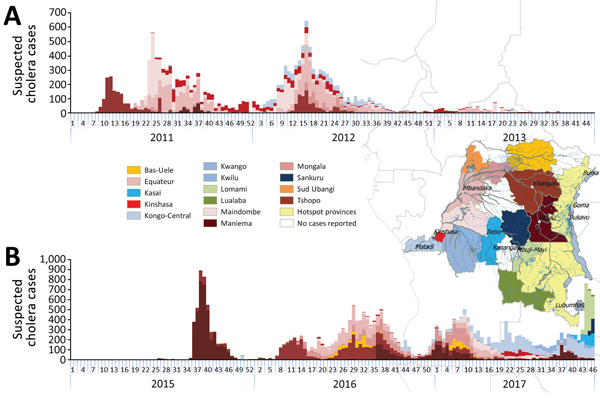
In 2017, the exacerbation of an ongoing countrywide cholera outbreak in the Democratic Republic of the Congo resulted in >53,000 reported cases and 1,145 deaths. To guide control measures, we analyzed the characteristics of cholera epidemiology in DRC on the basis of surveillance and cholera treatment center data for 2008-2017. The 2017 nationwide outbreak resulted from 3 distinct mechanisms: considerable increases in the number of cases in cholera-endemic areas, so-called hot spots, around the Great Lakes in eastern DRC; recurrent outbreaks progressing downstream along the Congo River; and spread along Congo River branches to areas that had been cholera-free for more than a decade. Case-fatality rates were higher in nonendemic areas and in the early phases of the outbreaks, possibly reflecting low levels of immunity and less appropriate prevention and treatment. Targeted use of oral cholera vaccine, soon after initial cases are diagnosed, could contribute to lower case-fatality rates.
2017 年,刚果民主共和国全国范围内霍乱疫情恶化,报告病例超过 53000 例,死亡 1145 例。为指导控制措施,我们根据 2008-2017 年的监测和霍乱治疗中心数据,分析了刚果民主共和国的霍乱流行特征。2017 年的全国性疫情是由以下 3 种不同机制引起的:刚果民主共和国东部大湖区附近霍乱流行地区,即所谓的热点地区,病例数量大幅增加;刚果河沿岸疫情反复发生;以及沿着刚果河支流传播到十年来一直没有霍乱的地区。在非流行地区和疫情早期,病死率更高,这可能反映了免疫力较低,预防和治疗措施不恰当。在确诊最初病例后,尽快有针对性地使用口服霍乱疫苗,可能有助于降低病死率。