Bompangue Didier, Vesenbeckh Silvan Manuel, Giraudoux Patrick, Castro Marcia, Muyembe Jean-Jacques, Kebela Ilunga Benoît, Murray Megan
Laboratoire Chrono-environnement, UMR6249, CNRS, University of Franche-Comté, Place Leclerc 25030 Besançon, France. Laboratory of Microbiology, Faculty of Medicine, University of Kinshasa, BP: 834, Kinshasa, Democratic Republic of Congo. Direction de Lutte contre la Maladie, Ministry of Public Health, Av. de la Justice 39, Gombe I, Kinshasa, Democratic Republic of Congo.; Harvard School of Public Health, Center for Communicable Disease Dynamics, 677 Huntington Avenue, Boston MA 02115, USA. Brigham and Women's Hospital, Division of Global Health Equity, 75 Francis Street, Boston MA 02115, USA; Laboratoire Chrono-environnement, UMR6249, CNRS, University of Franche-Comté, Place Leclerc 25030 Besançon, France; Harvard School of Public Health, Department of Global Health and Population, 677 Huntington Avenue, Boston MA 02115, USA; Laboratory of Microbiology, Faculty of Medicine, University of Kinshasa, BP: 834, Kinshasa, Democratic Republic of Congo; Direction de Lutte contre la Maladie, Ministry of Public Health, Av. de la Justice 39, Gombe I, Kinshasa, Democratic Republic of Congo and Brigham and Women's Hospital, Division of Global Health Equity, 75 Francis Street, Boston MA 02115, USA. Harvard School of Public Health, Department of Epidemiology, 677 Huntington Avenue, Boston MA 02115, USA.
PLoS Curr. 2012 Feb 17;4:RRN1310. doi: 10.1371/currents.RRN1310.
Cholera is an endemic disease in certain well-defined areas in the east of the Democratic Republic of Congo (DRC). The west of the country, including the mega-city Kinshasa, has been free of cases since mid 2001 when the last outbreak ended.
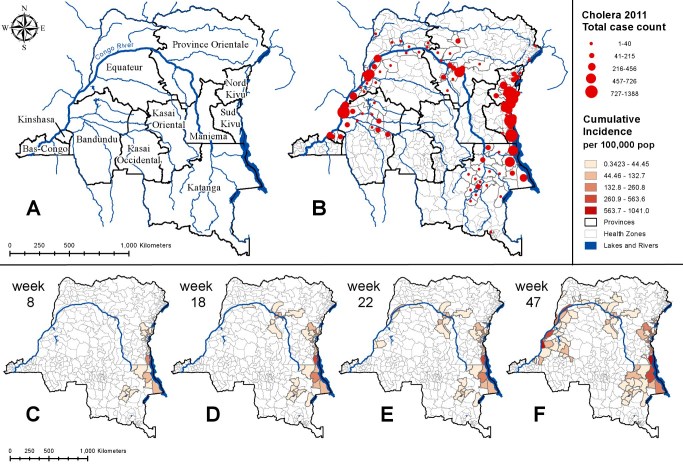
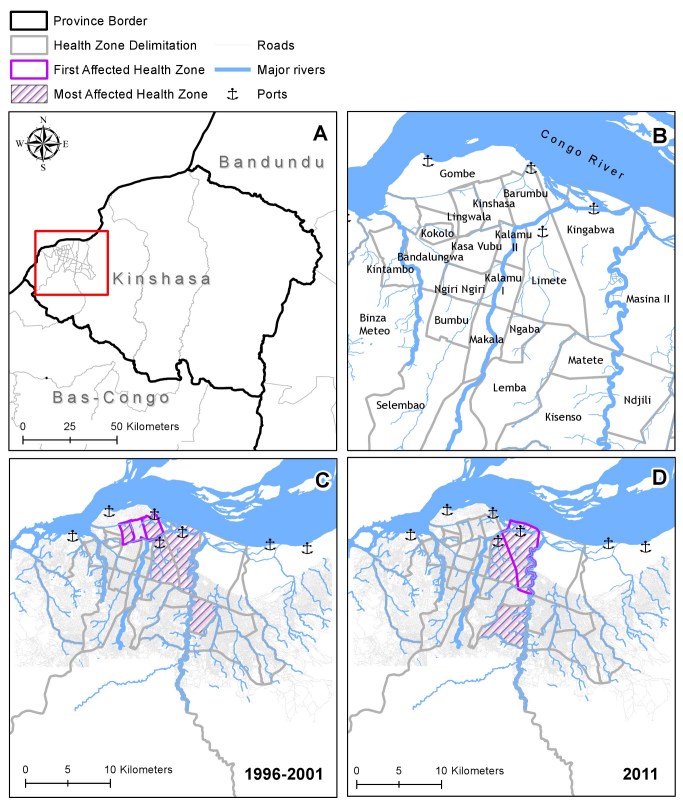
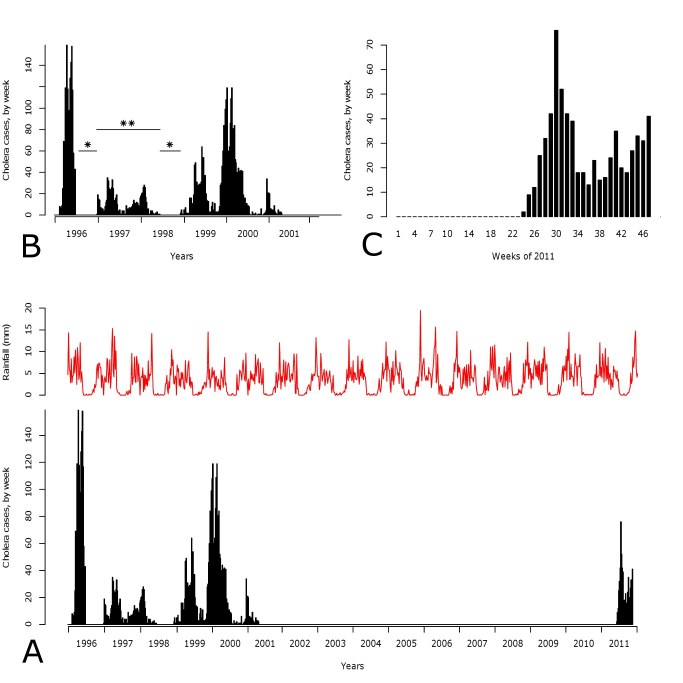
We used routinely collected passive surveillance data to construct epidemic curves of the cholera cases and map the spatio-temporal progress of the disease during the first 47 weeks of 2011. We compared the spatial distribution of disease spread to that which occurred in the last cholera epidemic in Kinshasa between 1996 and 2001. To better understand previous determinants of cholera spread in this region, we conducted a correlation analysis to assess the impact of rainfall on weekly health zone cholera case counts between December 1998 and March 2001 and a Generalized Linear Model (GLM) regression analysis to identify factors that have been associated with the most vulnerable health zones within Kinshasa between October 1998 and June 1999. In February 2011, cholera reemerged in a region surrounding Kisangani and gradually spread westwards following the course of the Congo River to Kinshasa, home to 10 million people. Ten sampled isolates were confirmed to be Vibrio cholerae O1, biotype El Tor, serotype Inaba, resistant to trimethoprim-sulfa, furazolidone, nalidixic acid, sulfisoxaole, and streptomycin, and intermediate resistant to Chloramphenicol. An analysis of a previous outbreak in Kinshasa shows that rainfall was correlated with case counts and that health zone population densities as well as fishing and trade activities were predictors of case counts.
Cholera is particularly difficult to tackle in the DRC. Given the duration of the rainy season and increased riverine traffic from the eastern provinces in late 2011, we expect further increases in cholera in the coming months and especially within the mega-city Kinshasa. We urge all partners involved in the response to remain alert.Didier Bompangue and Silvan Vesenbeckh contributed equally to this work. *corresponding author: Silvan Vesenbeckh, Harvard School of Public Health (vesenbeckh@gmail.com)Didier Bompangue is Associate Professor in the Department of Microbiology (University of Kinshasa) andEpidemiologist in the DRC Ministry of Health. He was involved in the investigations of the described outbreak since February 2011.
霍乱是刚果民主共和国(DRC)东部某些明确界定地区的一种地方病。该国西部,包括大城市金沙萨,自2001年年中最后一次疫情结束以来一直没有病例。
我们使用常规收集的被动监测数据构建霍乱病例的流行曲线,并绘制2011年最初47周内该疾病的时空进展情况。我们将疾病传播的空间分布与1996年至2001年金沙萨上一次霍乱疫情期间的情况进行了比较。为了更好地了解该地区先前霍乱传播的决定因素,我们进行了相关性分析,以评估1998年12月至2001年3月期间降雨对每周卫生区霍乱病例数的影响,并进行了广义线性模型(GLM)回归分析,以确定1998年10月至1999年6月期间金沙萨最脆弱卫生区内与病例数相关的因素。2011年2月,霍乱在基桑加尼周边地区再次出现,并沿着刚果河向西逐渐蔓延至拥有1000万人口的金沙萨。十个采样分离株被确认为霍乱弧菌O1型,埃尔托生物型,稻叶血清型,对甲氧苄啶 -磺胺、呋喃唑酮、萘啶酸、磺胺异恶唑和链霉素耐药,对氯霉素中度耐药。对金沙萨先前一次疫情的分析表明,降雨与病例数相关,卫生区人口密度以及渔业和贸易活动是病例数的预测因素。
在刚果民主共和国,霍乱特别难以应对。鉴于雨季的持续时间以及2011年末来自东部省份的内河运输增加,我们预计未来几个月霍乱病例数将进一步增加,尤其是在大城市金沙萨。我们敦促所有参与应对的伙伴保持警惕。迪迪埃·邦庞格和西尔万·韦森贝克对这项工作贡献相同。*通讯作者:西尔万·韦森贝克,哈佛公共卫生学院(vesenbeckh@gmail.com)迪迪埃·邦庞格是金沙萨大学微生物学系副教授,也是刚果民主共和国卫生部的流行病学家。自2011年2月以来,他参与了所述疫情的调查。