Wang Dongdong, Lu Jinmiao, Li Qin, Li Zhiping
Department of Pharmacy, Children's Hospital of Fudan University, Shanghai 201102, P.R. China.
Exp Ther Med. 2019 May;17(5):4023-4031. doi: 10.3892/etm.2019.7446. Epub 2019 Mar 27.
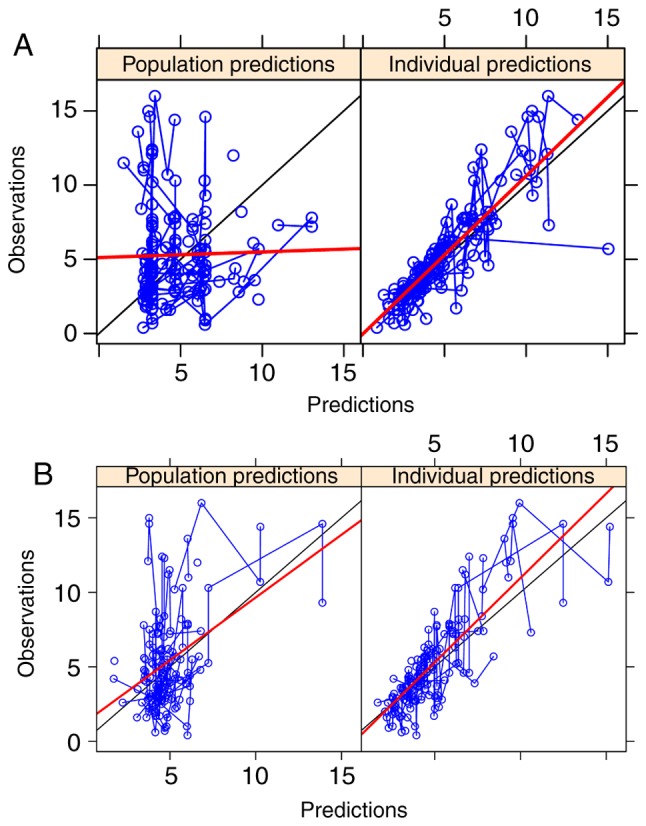
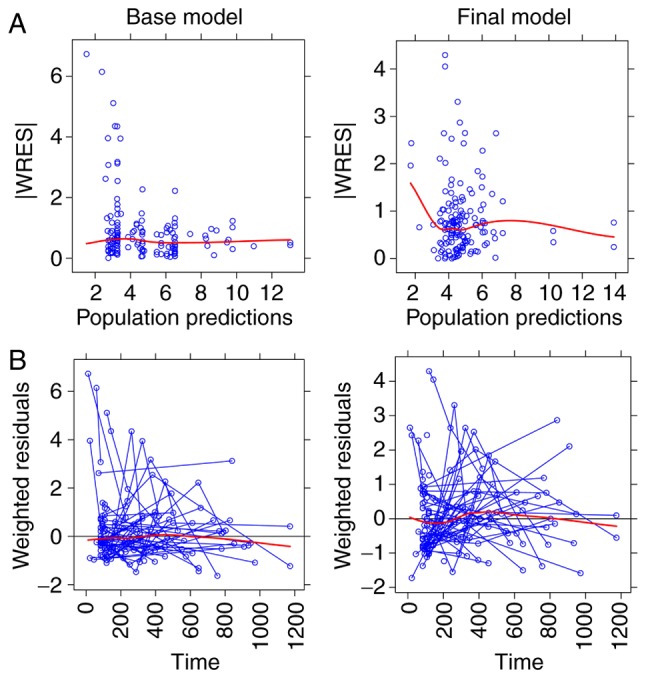
Different tacrolimus (TAC) population pharmacokinetic (PPK) models have been established in various pediatric disease populations. However, a TAC PPK model for pediatric refractory nephrotic syndrome (PRNS) has not been well characterized. The current study aimed to establish a TAC PPK model in Chinese PRNS and provide a summary of previous literature concerning TAC PPK models in different pediatric diseases. A total of 147 TAC conventional therapeutic drug monitoring (TDM) data from multiple blood samples obtained from 65 Chinese patients with PRNS were characterized using nonlinear mixed-effects modeling. The impacts of demographic features, biological characteristics and drug combination were evaluated. Model validation was assessed using the bootstrap method. A one-compartment model with first-order absorption and elimination was determined to be the most suitable model for TDM data in PRNS. The absorption rate constant (Ka) was set at 4.48 h. The typical values of apparent oral clearance (CL/F) and apparent volume of distribution (V/F) in the final model were 5.46 l/h and 57.1 l, respectively. The inter-individual variability of CL/F and V/F were 22.2 and 0.2%, respectively. The PPK equation for TAC was: CL/F = 5.46 × exponential function (EXP)(0.0323 × age) × EXP(-0.359 × cystatin-C) × EXP(0.148 × daily dose of TAC). No significant effects of covariates on V/F were observed. In conclusion, the current study developed and validated the first TAC PPK model for patients with PRNS. The study also provided a summary of previous literature concerning other TAC PPK models in different pediatric diseases.
不同的他克莫司(TAC)群体药代动力学(PPK)模型已在各种儿科疾病群体中建立。然而,针对小儿难治性肾病综合征(PRNS)的TAC PPK模型尚未得到充分表征。本研究旨在建立中国PRNS患者的TAC PPK模型,并总结先前关于不同儿科疾病中TAC PPK模型的文献。使用非线性混合效应模型对来自65例中国PRNS患者的多个血样中获得的147个TAC常规治疗药物监测(TDM)数据进行了表征。评估了人口统计学特征、生物学特征和药物组合的影响。使用自抽样法进行模型验证。确定具有一级吸收和消除的单室模型是PRNS中TDM数据最合适的模型。吸收速率常数(Ka)设定为4.48 h。最终模型中表观口服清除率(CL/F)和表观分布容积(V/F)的典型值分别为5.46 l/h和57.1 l。CL/F和V/F的个体间变异性分别为22.2%和0.2%。TAC的PPK方程为:CL/F = 5.46×指数函数(EXP)(0.0323×年龄)×EXP(-0.359×胱抑素-C)×EXP(0.148×TAC每日剂量)。未观察到协变量对V/F有显著影响。总之,本研究开发并验证了首个针对PRNS患者的TAC PPK模型。该研究还总结了先前关于不同儿科疾病中其他TAC PPK模型的文献。