Division of Gastroenterology and Hepatology, Department of Internal Medicine, University of Michigan School of Medicine, Ann Arbor, Michigan, USA.
Am J Gastroenterol. 2019 Jul;114(7):1163-1171. doi: 10.14309/ajg.0000000000000200.
Small intestinal bacterial overgrowth (SIBO) is often present in patients with chronic pancreatitis (CP) with persistent steatorrhea, despite pancreatic enzyme replacement therapy. Overall prevalence of SIBO, diagnosed by glucose breath test (GBT), varies between 0% and 40% but 0%-21% in those without upper gastrointestinal (GI) surgery. We investigated the prevalence and nonsurgical independent predictors of SIBO in CP without upper GI surgery.
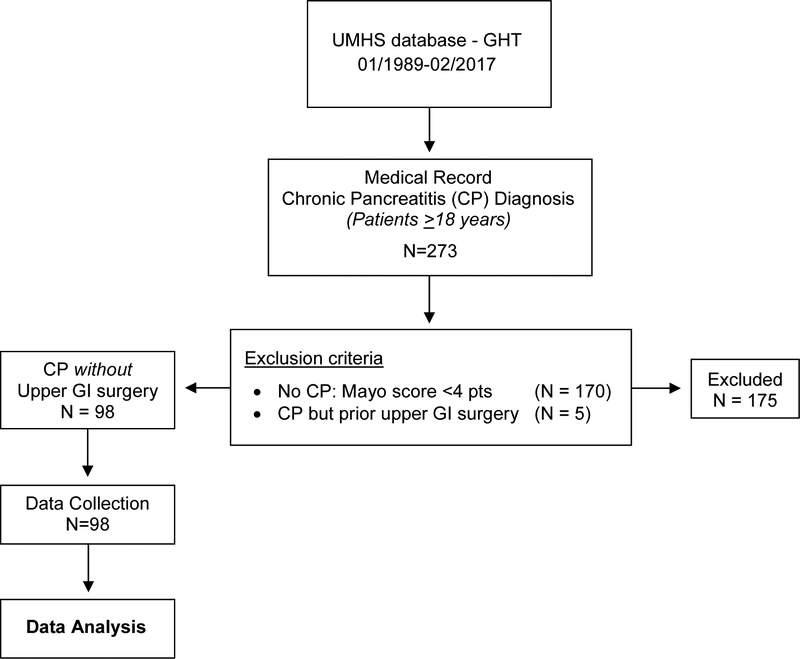
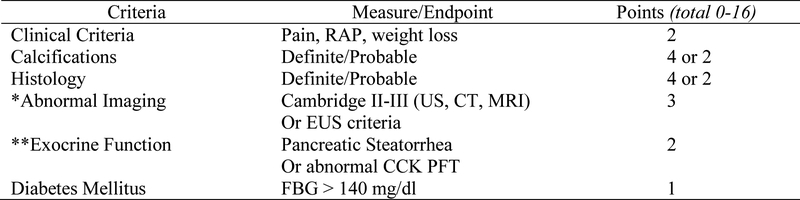
Two hundred seventy-three patients ≥18 years old had a presumptive diagnosis of CP and a GBT between 1989 and 2017. We defined CP by Mayo score (0-16) ≥4 and a positive GBT for SIBO by Rome consensus criteria and retrospectively collected data for 5 a priori variables (age, opiates, alcohol use, diabetes mellitus (DM), gastroparesis) and 41 investigational variables (demographics, GI symptoms, comorbidities, CP etiologies and cofactors, CP symptom duration, Mayo score and nondiabetes components, and biochemical variables).
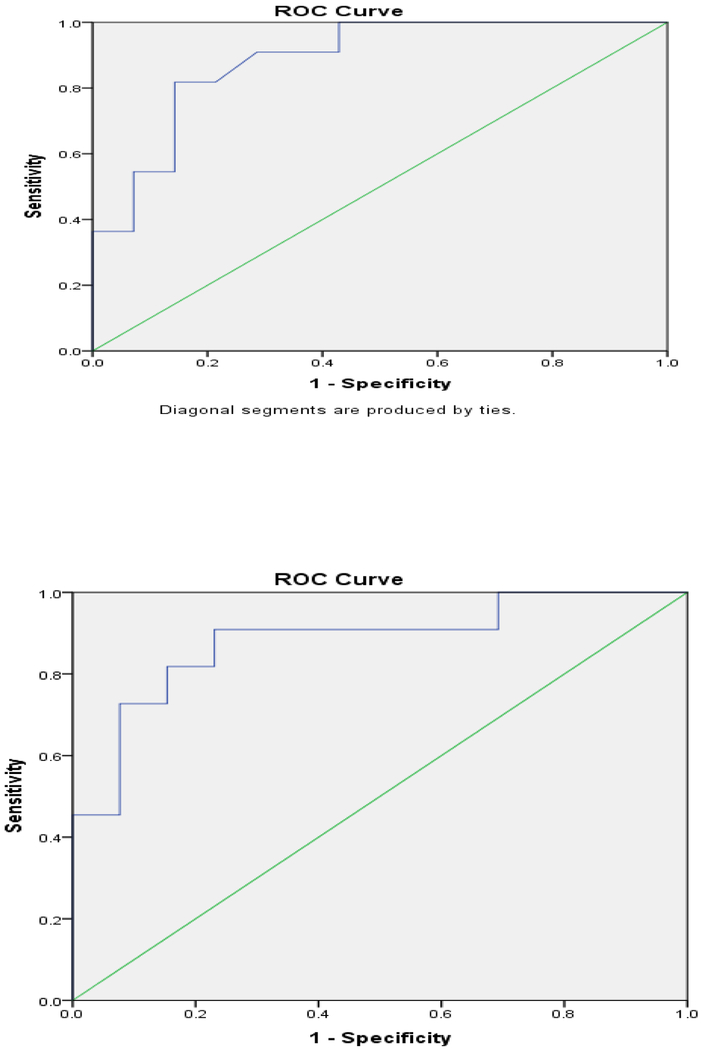
Ninety-eight of 273 patients had definite CP and 40.8% had SIBO. Five of 46 variables predicted SIBO: opiates, P = 0.005; DM, P = 0.04; total Mayo score, P < 0.05; zinc, P = 0.005; and albumin, P < 0.05). Multivariable analysis of 3 noncorrelated variables identified zinc level (odds ratio = 0.0001; P = 0.03) as the sole independent predictor of SIBO (model C-statistic = 0.89; P < 0.001).
SIBO, diagnosed by GBT, occurs in 40.8% of patients with CP without upper GI surgery. In patients with CP, markers of more severe CP (low zinc level, DM and increased Mayo score) and opiate use should raise clinical suspicion for SIBO, particularly in patients with persistent steatorrhea or weight loss despite pancreatic enzyme replacement therapy.
尽管进行了胰酶替代治疗,患有慢性胰腺炎(CP)且持续脂肪泻的患者常伴有小肠细菌过度生长(SIBO)。通过葡萄糖呼气试验(GBT)诊断的 SIBO 的总体患病率在 0%至 40%之间,但在上消化道(GI)手术中为 0%至 21%。我们研究了未经上 GI 手术的 CP 中 SIBO 的患病率和非手术独立预测因子。
1989 年至 2017 年间,共有 273 名年龄≥18 岁的患者有 CP 的推测诊断和 GBT。我们通过 Mayo 评分(0-16)≥4 和罗马共识标准的阳性 GBT 来定义 CP,并回顾性收集了 5 个先验变量(年龄,阿片类药物,酒精使用,糖尿病(DM),胃轻瘫)和 41 个研究变量(人口统计学,GI 症状,合并症,CP 病因和伴随因素,CP 症状持续时间,Mayo 评分和非糖尿病成分以及生化变量)。
273 例患者中有 98 例有明确的 CP,有 40.8%的患者有 SIBO。有 5 个变量可预测 SIBO:阿片类药物,P = 0.005;DM,P = 0.04;总 Mayo 评分,P <0.05;锌,P = 0.005;白蛋白,P <0.05)。对 3 个不相关变量的多变量分析确定了锌水平(优势比= 0.0001;P = 0.03)是 SIBO 的唯一独立预测因子(模型 C 统计量= 0.89;P <0.001)。
通过 GBT 诊断的 SIBO 发生在 40.8%未经上 GI 手术的 CP 患者中。在 CP 患者中,更严重 CP 的标志物(低锌水平,DM 和增加的 Mayo 评分)和阿片类药物的使用应引起对 SIBO 的临床怀疑,尤其是在持续脂肪泻或体重减轻的患者中尽管进行了胰酶替代治疗。