Butler-Xu Yiqing Shirley, Marietta Michael, Zahra Amir, TenNapel Mindi, Mitchell Melissa
Department of Radiation Oncology, University of Kansas Cancer Center, Kansas City, Kansas.
Department of Radiation Oncology, University of Southern California, Los Angeles, California.
Adv Radiat Oncol. 2018 Nov 1;4(2):261-267. doi: 10.1016/j.adro.2018.10.005. eCollection 2019 Apr-Jun.
Hypofractionated radiation therapy (HFRT) remains underused, despite multiple randomized trials showing the equivalence of HFRT to conventional fractionated radiation therapy (CFRT). We sought to retrospectively review the relationship between breast volume and toxicity for HFRT versus CFRT.
Data from 114 patients who received a diagnosis of early stage breast cancer and were treated with lumpectomy and whole breast radiation alone were reviewed. Breast cancer laterality, stage, grade, estrogen/progesterone receptor and human epidermal growth factor receptor 2 status, and systemic therapy use were recorded. Length of follow-up was calculated using the last day of radiation treatment and the date of the most recent follow-up.
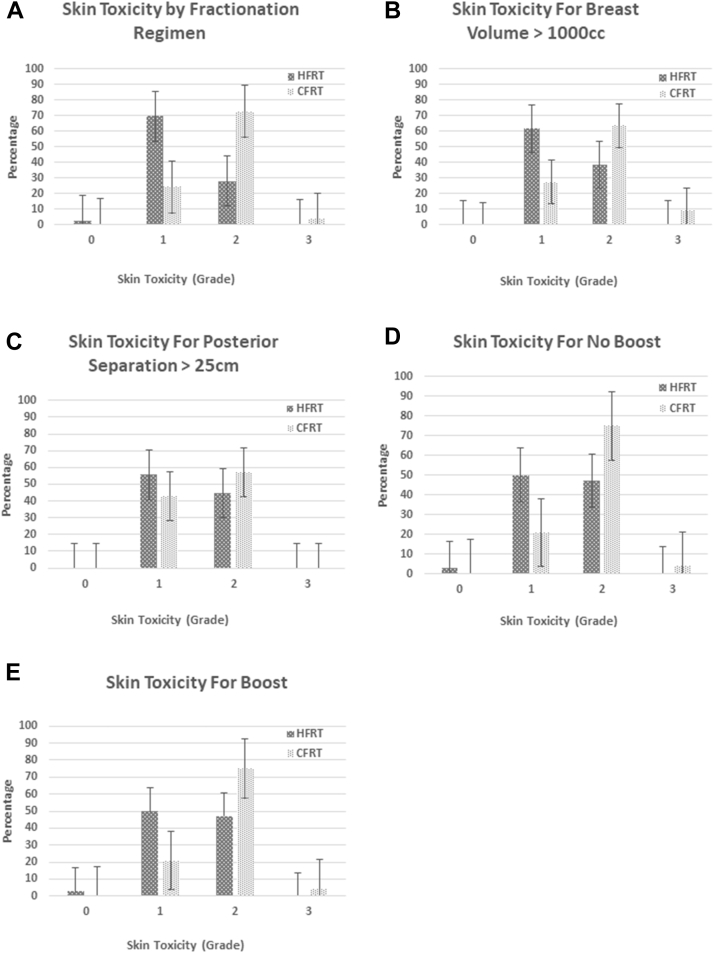
The median follow-up was 42 months. A total of 83 patients were treated with HFRT and 31 with CFRT. Rates of grade ≥2 skin toxicity were significantly higher in patients undergoing CFRT compared with HFRT (76% vs 28%; < .0001). In a subset of patients with breast volume ≥1000 cm, grade ≥2 skin toxicity trended higher for CFRT patients (73% vs 38%; = .057). For posterior separation >25 cm, the percentage of patients with grade 2 skin toxicity was 43% for HFRT versus 57% for CFRT ( = .67). The volume of breast tissue receiving >105% of the total prescription dose, including boost, was not significantly different for HFRT versus CFRT ( = .70).
Use of HFRT resulted in lower acute skin toxicity rates compared with CFRT. Large breast size (volume ≥1000 cm) was associated with lower acute grade 2 toxicity with the use of HFRT despite achieving similar dosimetry compared with CFRT.
尽管多项随机试验表明大分割放疗(HFRT)与传统分割放疗(CFRT)等效,但大分割放疗的使用仍未得到充分利用。我们试图回顾性分析HFRT与CFRT的乳腺体积与毒性之间的关系。
回顾了114例被诊断为早期乳腺癌且仅接受保乳手术和全乳放疗的患者的数据。记录乳腺癌的患侧、分期、分级、雌激素/孕激素受体和人表皮生长因子受体2状态以及全身治疗的使用情况。随访时间通过放疗的最后一天和最近一次随访日期计算得出。
中位随访时间为42个月。共有83例患者接受了HFRT治疗,31例接受了CFRT治疗。与HFRT相比,接受CFRT的患者≥2级皮肤毒性发生率显著更高(76%对28%;P<0.0001)。在乳腺体积≥1000cm³的患者亚组中,CFRT患者的≥2级皮肤毒性有升高趋势(73%对38%;P = 0.057)。对于后缘间距>25 cm,HFRT患者2级皮肤毒性的百分比为43%,而CFRT患者为57%(P = 0.67)。接受总处方剂量(包括增量剂量)>105% 的乳腺组织体积,HFRT与CFRT相比无显著差异(P = 0.70)。
与CFRT相比,使用HFRT导致急性皮肤毒性发生率更低。尽管与CFRT相比剂量测定相似,但大乳房尺寸(体积≥1000cm³)与使用HFRT时较低的急性2级毒性相关。