Institute of Cardiovascular and Medical Sciences (P.W., S.P., C.W., N.S.), University of Glasgow, United Kingdom.
MRC Population Health Research Unit, Clinical Trial Service Unit and Epidemiological Studies Unit (D. Preiss), University of Oxford, United Kingdom.
Circulation. 2019 Jun 11;139(24):2754-2764. doi: 10.1161/CIRCULATIONAHA.118.038529. Epub 2019 Apr 24.
There is great interest in widening the use of high-sensitivity cardiac troponins for population cardiovascular disease (CVD) and heart failure screening. However, it is not clear whether cardiac troponin T (cTnT) and troponin I (cTnI) are equivalent measures of risk in this setting. We aimed to compare and contrast (1) the association of cTnT and cTnI with CVD and non-CVD outcomes, and (2) their determinants in a genome-wide association study.
High-sensitivity cTnT and cTnI were measured in serum from 19 501 individuals in Generation Scotland Scottish Family Health Study. Median follow-up was 7.8 years (quartile 1 to quartile 3, 7.1-9.2). Associations of each troponin with a composite CVD outcome (1177 events), CVD death (n=266), non-CVD death (n=374), and heart failure (n=216) were determined by using Cox models. A genome-wide association study was conducted using a standard approach developed for the cohort.
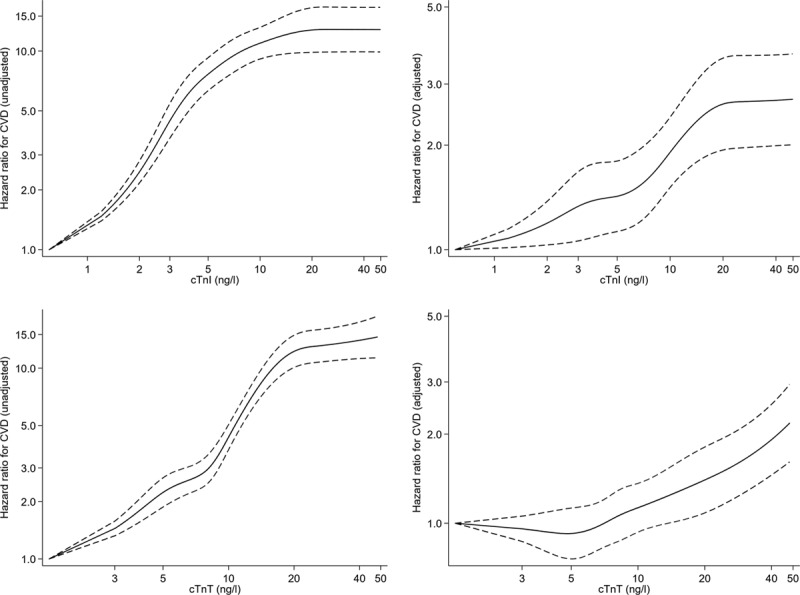
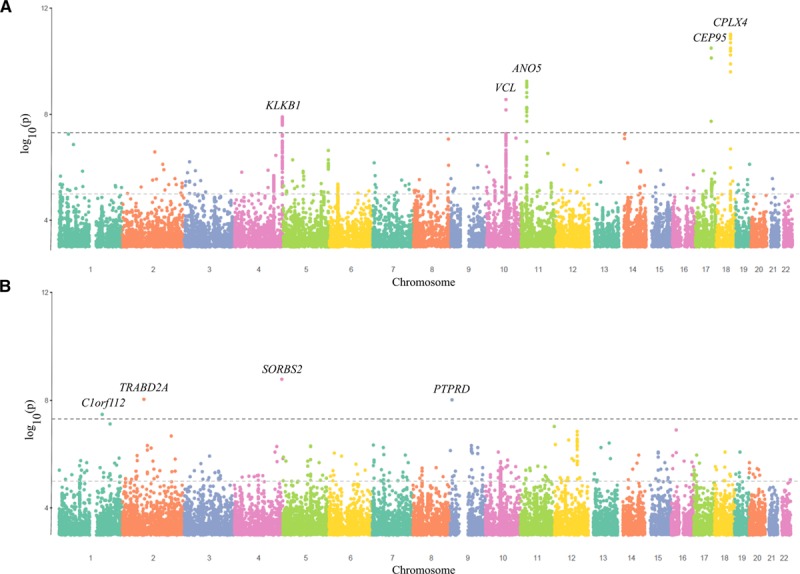
Both cTnI and cTnT were strongly associated with CVD risk in unadjusted models. After adjusting for classical risk factors, the hazard ratio for a 1 SD increase in log transformed troponin was 1.24 (95% CI, 1.17-1.32) and 1.11 (1.04-1.19) for cTnI and cTnT, respectively; ratio of hazard ratios 1.12 (1.04-1.21). cTnI, but not cTnT, was associated with myocardial infarction and coronary heart disease. Both cTnI and cTnT had strong associations with CVD death and heart failure. By contrast, cTnT, but not cTnI, was associated with non-CVD death; ratio of hazard ratios 0.77 (0.67-0.88). We identified 5 loci (53 individual single-nucleotide polymorphisms) that had genome-wide significant associations with cTnI, and a different set of 4 loci (4 single-nucleotide polymorphisms) for cTnT.
The upstream genetic causes of low-grade elevations in cTnI and cTnT appear distinct, and their associations with outcomes also differ. Elevations in cTnI are more strongly associated with some CVD outcomes, whereas cTnT is more strongly associated with the risk of non-CVD death. These findings help inform the selection of an optimal troponin assay for future clinical care and research in this setting.
人们对扩大高敏心肌肌钙蛋白在人群心血管疾病(CVD)和心力衰竭筛查中的应用非常感兴趣。然而,目前尚不清楚在这种情况下,肌钙蛋白 T(cTnT)和肌钙蛋白 I(cTnI)是否是风险的等效衡量指标。我们旨在比较和对比(1)cTnT 和 cTnI 与 CVD 和非 CVD 结局的相关性,以及(2)它们在全基因组关联研究中的决定因素。
在苏格兰基因世代研究的 19501 名个体的血清中测量了高敏 cTnT 和 cTnI。中位随访时间为 7.8 年(四分位距 1 至 3 分位距,7.1-9.2)。使用 Cox 模型确定了每种肌钙蛋白与复合 CVD 结局(1177 例事件)、CVD 死亡(n=266)、非 CVD 死亡(n=374)和心力衰竭(n=216)的相关性。使用为该队列开发的标准方法进行了全基因组关联研究。
cTnI 和 cTnT 在未调整模型中均与 CVD 风险密切相关。在调整了经典危险因素后,cTn 对数转换后每增加 1 SD 的风险比为 1.24(95%CI,1.17-1.32)和 1.11(1.04-1.19),分别为 cTnI 和 cTnT;风险比比值为 1.12(1.04-1.21)。cTnI 与心肌梗死和冠心病相关,但 cTnT 无此相关性。cTnI 和 cTnT 均与 CVD 死亡和心力衰竭密切相关。相比之下,cTnT 与非 CVD 死亡相关,但 cTnI 无此相关性;风险比比值为 0.77(0.67-0.88)。我们确定了 5 个与 cTnI 具有全基因组显著关联的基因座(53 个个体单核苷酸多态性),以及 4 个与 cTnT 具有全基因组显著关联的基因座(4 个单核苷酸多态性)。
cTnI 和 cTnT 低度升高的上游遗传原因似乎不同,它们与结局的相关性也不同。cTnI 升高与某些 CVD 结局的相关性更强,而 cTnT 升高与非 CVD 死亡的风险相关性更强。这些发现有助于为今后在这一环境下的临床护理和研究选择最佳的肌钙蛋白检测方法提供信息。