Memorial Sloan Kettering Cancer Center, United States.
Memorial Sloan Kettering Cancer Center, United States.
Radiother Oncol. 2019 Jun;135:19-24. doi: 10.1016/j.radonc.2019.02.014. Epub 2019 Mar 5.
PURPOSE/OBJECTIVE: Hypofractionated radiotherapy (HRT) regimens for prostate cancer are emerging, but tolerance doses for late adverse events are scarce. The purpose of this study is to define dose-volume predictors for late gastrointestinal and genitourinary (GI and GU) toxicities after HRT in the multi-center NRG Oncology/RTOG 0415 low-risk prostate cancer trial (N = 521).
MATERIAL/METHODS: Treatment in the studied HRT arm was delivered as 70 Gy at 2.5 Gy/fraction with 3D-CRT/IMRT (N = 108/413). At a median follow-up of 5.9 years, the crude late ≥Grade 2 GI and GU toxicities were 19% and 29%, respectively. For modeling, the complete HRT cohort was randomly split into training and validation (70% and 30%; preserved toxicity rates). Within training, dose-response modeling was based on dose-volume cut-points (EQD2Gy; bladder/rectum: α/β = 6 Gy/3Gy), age, acute ≥Grade 2 toxicity, and treatment technique using univariate and multivariate logistic regression on bootstrapping (UVA and MVA). Candidate predictors were determined at p ≤ 0.05, and the selected MVA models were explored on validation where model generalizability was judged if the area under the receiver-operating curve in validation (AUC) was within AUC ± SD with p ≤ 0.05, and with an Hosmer-Lemeshow p-value (p) > 0.05.
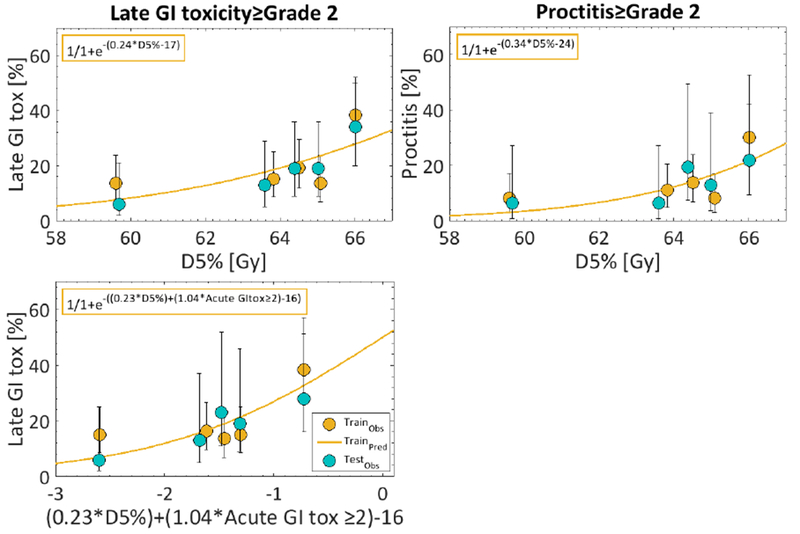
Three candidate predictors were suggested for late GI toxicity: the minimum dose to the hottest 5% rectal volume (D5%[Gy]), the absolute rectal volume <35 Gy, and acute GI toxicity (AUC = 0.59-0.63; p = 0.02-0.04). The two generalizable MVA models, i.e., D5%[Gy] with or without acute GI toxicity (AUC = 0.64, 0.65; p = 0.01, 0.03; p = 0.45-0.56), suggest that reducing late GI toxicity from 20% to 10% would require reducing D5%[Gy] from ≤65 Gy to ≤62 Gy (logistic function argument: 17+(0.24D5%[Gy])). Acute GU toxicity showed only a trend to predict late GU toxicity (AUC = 0.57; p = 0.07).
Late GI toxicity, following moderate HRT for low-risk prostate cancer, increases with higher doses to small rectal volumes. This work provides quantitative evidence that limiting small rectal dose 'hotspots' in clinical practice of such HRT regimens is likely to further reduce the associated rates of GI toxicity.
前列腺癌的分割放疗方案正在不断涌现,但对于晚期不良反应的耐受剂量却知之甚少。本研究的目的是在 NRG Oncology/RTOG 0415 低危前列腺癌试验(N=521)中,为多中心 NRG Oncology/RTOG 0415 低危前列腺癌试验中的晚期胃肠道和泌尿生殖系统(GI 和 GU)毒性的分割放疗(HRT)定义剂量-体积预测因子。
研究中的 HRT 臂的治疗方法为 70Gy 分 2.5Gy/次,采用 3D-CRT/IMRT(N=108/413)。在中位随访 5.9 年后,晚期≥2 级胃肠道和泌尿生殖系统毒性的发生率分别为 19%和 29%。为了建模,完整的 HRT 队列被随机分为训练集和验证集(70%和 30%;保留毒性率)。在训练集中,剂量反应建模基于剂量-体积截断点(EQD2Gy;膀胱/直肠:α/β=6Gy/3Gy)、年龄、急性≥2 级毒性和治疗技术,采用单变量和多变量逻辑回归进行 bootstrap 分析(UVA 和 MVA)。候选预测因子在 p≤0.05 时确定,所选 MVA 模型在验证集中进行了探索,如果验证集中的接受者操作特征曲线下面积(AUC)在 AUC±SD 范围内(p≤0.05),并且 Hosmer-Lemeshow p 值(p)>0.05,则判断模型的通用性。
有三个候选预测因子被建议用于晚期胃肠道毒性: hottest 5%直肠体积(D5%[Gy])的最小剂量、直肠体积<35Gy 的绝对体积和急性胃肠道毒性(AUC=0.59-0.63;p=0.02-0.04)。两个可推广的 MVA 模型,即 D5%[Gy]与急性胃肠道毒性(AUC=0.64,0.65;p=0.01,0.03;p=0.45-0.56),表明将晚期胃肠道毒性从 20%降低到 10%需要将 D5%[Gy]从≤65Gy 降低到≤62Gy(逻辑函数参数:17+(0.24D5%[Gy]))。急性 GU 毒性仅显示出预测晚期 GU 毒性的趋势(AUC=0.57;p=0.07)。
对于低危前列腺癌,采用中度 HRT 治疗后,晚期胃肠道毒性随直肠小体积的高剂量而增加。本研究提供了定量证据,表明在这种 HRT 方案的临床实践中限制小直肠剂量的“热点”,可能会进一步降低相关的胃肠道毒性发生率。