Kumar Aravin, Liu Nan, Koh Zhi Xiong, Chiang Jayne Jie Yi, Soh Yuda, Wong Ting Hway, Ho Andrew Fu Wah, Tagami Takashi, Fook-Chong Stephanie, Ong Marcus Eng Hock
1Yong Loo Lin School of Medicine, National University of Singapore, Singapore, Singapore.
2Health Services Research Centre, Singapore Health Services, Academia, 20 College Road, Singapore, 169856 Singapore.
Burns Trauma. 2019 Apr 18;7:12. doi: 10.1186/s41038-019-0147-2. eCollection 2019.
Triage trauma scores are utilised to determine patient disposition, interventions and prognostication in the care of trauma patients. Heart rate variability (HRV) and heart rate complexity (HRC) reflect the autonomic nervous system and are derived from electrocardiogram (ECG) analysis. In this study, we aimed to develop a model incorporating HRV and HRC, to predict the need for life-saving interventions (LSI) in trauma patients, within 24 h of emergency department presentation.
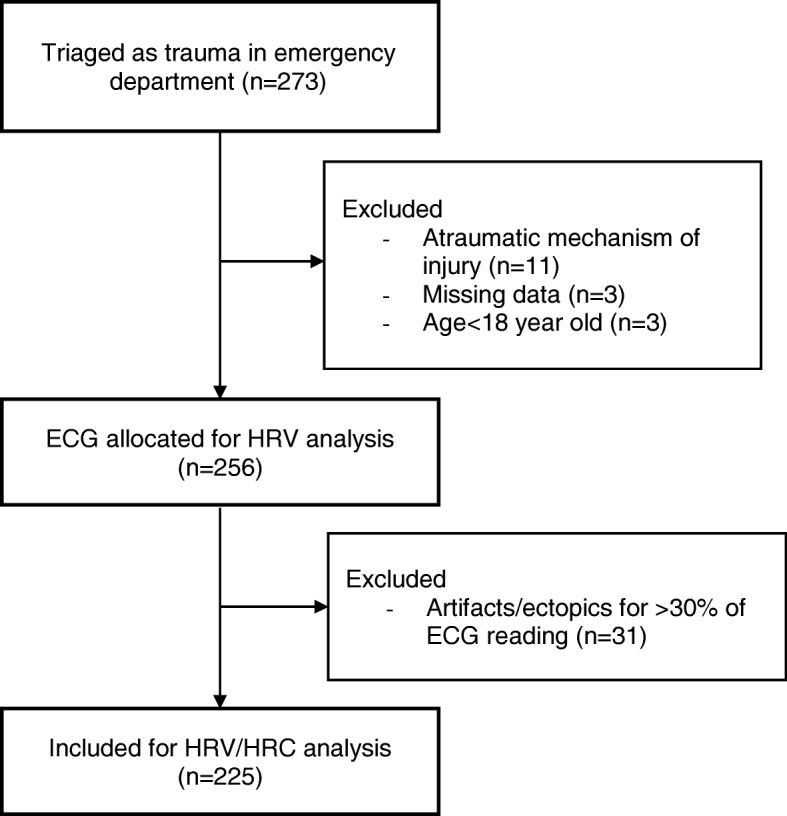
We included adult trauma patients (≥ 18 years of age) presenting at the emergency department of Singapore General Hospital between October 2014 and October 2015. We excluded patients who had non-sinus rhythms and larger proportions of artefacts and/or ectopics in ECG analysis. We obtained patient demographics, laboratory results, vital signs and outcomes from electronic health records. We conducted univariate and multivariate analyses for predictive model building.
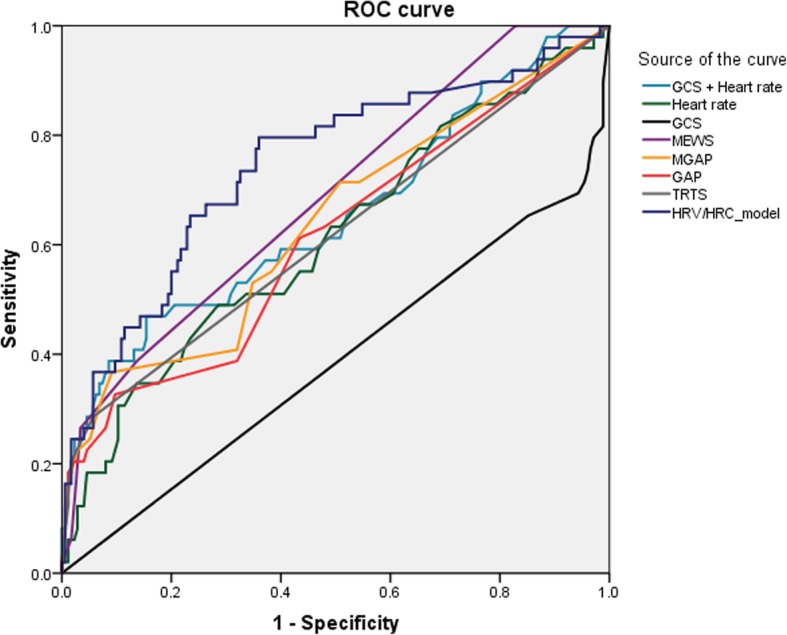
Two hundred and twenty-five patients met inclusion criteria, in which 49 patients required LSIs. The LSI group had a higher proportion of deaths (10, 20.41% vs 1, 0.57%, < 0.001). In the LSI group, the mean of detrended fluctuation analysis (DFA)-α1 (1.24 vs 1.12, = 0.045) and the median of DFA-α2 (1.09 vs 1.00, = 0.027) were significantly higher. Multivariate stepwise logistic regression analysis determined that a lower Glasgow Coma Scale, a higher DFA-α1 and higher DFA-α2 were independent predictors of requiring LSIs. The area under the curve (AUC) for our model (0.75, 95% confidence interval, 0.66-0.83) was higher than other scoring systems and selected vital signs.
An HRV/HRC model outperforms other triage trauma scores and selected vital signs in predicting the need for LSIs but needs to be validated in larger patient populations.
分诊创伤评分用于确定创伤患者护理中的患者处置、干预措施和预后。心率变异性(HRV)和心率复杂性(HRC)反映自主神经系统,可通过心电图(ECG)分析得出。在本研究中,我们旨在开发一个纳入HRV和HRC的模型,以预测创伤患者在急诊科就诊后24小时内对挽救生命干预措施(LSI)的需求。
我们纳入了2014年10月至2015年10月期间在新加坡总医院急诊科就诊的成年创伤患者(≥18岁)。我们排除了心电图分析中存在非窦性心律以及较大比例伪迹和/或异位心律的患者。我们从电子健康记录中获取患者的人口统计学信息、实验室检查结果、生命体征和结局。我们进行单变量和多变量分析以构建预测模型。
225名患者符合纳入标准,其中49名患者需要LSI。LSI组的死亡比例更高(10例,20.41%对1例,0.57%,<0.001)。在LSI组中,去趋势波动分析(DFA)-α1的平均值(1.24对1.12,P = 0.045)和DFA-α2的中位数(1.09对1.00,P = 0.027)显著更高。多变量逐步逻辑回归分析确定,较低的格拉斯哥昏迷量表评分、较高的DFA-α1和较高的DFA-α2是需要LSI的独立预测因素。我们模型的曲线下面积(AUC)为0.75(95%置信区间,0.66 - 0.83),高于其他评分系统和选定的生命体征。
在预测对LSI的需求方面,HRV/HRC模型优于其他分诊创伤评分和选定的生命体征,但需要在更大的患者群体中进行验证。