Hislop Patrick, Sakata Kentaro, Ackland David C, Gotmaker Robert, Evans Matthew C
Department of Biomedical Engineering, University of Melbourne, Parkville, Australia.
Melbourne Orthopaedic Group, Windsor, Australia.
Orthop J Sports Med. 2019 Apr 17;7(4):2325967119836751. doi: 10.1177/2325967119836751. eCollection 2019 Apr.
It is important to restore horizontal and vertical stability to the acromioclavicular (AC) joint when treating dislocations of this joint. Most surgical stabilization techniques of the AC joint have primarily addressed the coracoclavicular ligament complex; however, these techniques may not satisfactorily restore horizontal stability to the AC joint.
To evaluate the strength and bidirectional stability of 3 AC joint stabilizing techniques in a cadaveric model.
Controlled laboratory study.
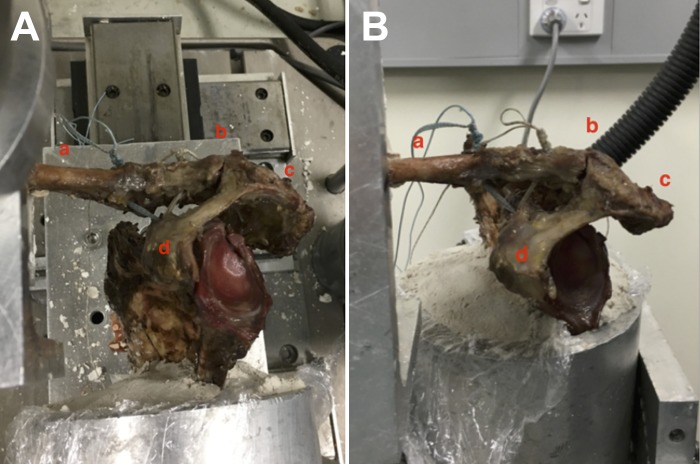
A total of 24 cadaveric shoulders were randomly allocated to 3 treatment groups. For each group, a standardized AC joint stabilizing procedure was performed, and the specimens were potted for mechanical testing. The following reconstruction techniques were used: a single clavicular tunnel for group A, a double clavicular tunnel for group B, and a double clavicular tunnel plus suture fixation across the AC joint for group C. The specimens underwent cyclic loading in the horizontal and vertical planes and then load to failure. Eight control specimens also underwent cyclic loading in both planes. Construct stiffness during cyclic loading, change in displacement after cyclic loading in both planes, load to failure in the vertical plane, and mode of failure were evaluated, and stiffness was compared among the treatment groups as well as with a control group.
There was a decrease in joint stiffness for all groups, including controls, during the cyclic loading. Compared with controls, all 3 treatment groups demonstrated equivalent stiffness and displacement in the vertical plane. In the horizontal plane, all 3 treatment groups demonstrated decreased stiffness, increased displacement, or both when compared with controls. When groups were compared, no treatment arm proved superior regarding stiffness or displacement in either plane. Load-to-failure testing of the 3 treatment groups in the vertical plane demonstrated construct strength and stiffness comparable with reports for the native AC joint. The mode of failure was predominantly fracture at the point of fixation to the testing apparatus.
There was no difference in bidirectional strength and stability between the single- and double-clavicular tunnel techniques of coracoclavicular reconstruction. The addition of a stabilizing suture across the AC joint does not improve horizontal stability in the absence of repair of the AC joint capsule and deltotrapezial fascia.
This laboratory study provides further evidence of the importance of the AC joint capsule and associated soft tissues in affording horizontal stability to that joint. Information from this and subsequent studies utilizing a bidirectional model can influence the choice of surgical procedure in the clinical treatment of AC joint dislocations.
治疗肩锁关节脱位时,恢复该关节的水平和垂直稳定性很重要。大多数肩锁关节手术稳定技术主要针对喙锁韧带复合体;然而,这些技术可能无法令人满意地恢复肩锁关节的水平稳定性。
在尸体模型中评估3种肩锁关节稳定技术的强度和双向稳定性。
对照实验室研究。
将24具尸体肩部随机分为3个治疗组。对每组进行标准化的肩锁关节稳定手术,将标本装入盆中进行力学测试。使用以下重建技术:A组为单锁骨隧道,B组为双锁骨隧道,C组为双锁骨隧道加肩锁关节缝合固定。标本在水平和垂直平面上进行循环加载,然后加载至破坏。8个对照标本也在两个平面上进行循环加载。评估循环加载期间的结构刚度、两个平面循环加载后的位移变化、垂直平面的破坏载荷以及破坏模式,并比较治疗组与对照组之间的刚度。
包括对照组在内的所有组在循环加载期间关节刚度均降低。与对照组相比,所有3个治疗组在垂直平面上表现出相当的刚度和位移。在水平平面上,与对照组相比,所有3个治疗组均表现出刚度降低、位移增加或两者兼而有之。当比较各治疗组时,没有一个治疗组在任一平面的刚度或位移方面表现更优。3个治疗组在垂直平面上的破坏载荷测试表明,结构强度和刚度与天然肩锁关节的报道相当。破坏模式主要是在固定到测试设备的点处骨折。
喙锁重建的单锁骨隧道技术和双锁骨隧道技术在双向强度和稳定性方面没有差异。在未修复肩锁关节囊和三角肌斜方肌筋膜的情况下,在肩锁关节上加用稳定缝线并不能改善水平稳定性。
这项实验室研究进一步证明了肩锁关节囊及相关软组织在为该关节提供水平稳定性方面的重要性。来自这项研究以及随后使用双向模型的研究信息可影响肩锁关节脱位临床治疗中手术方法的选择。

