Astellas Pharma Inc., Tokyo, Japan.
Br J Clin Pharmacol. 2019 Aug;85(8):1808-1819. doi: 10.1111/bcp.13972. Epub 2019 Jun 20.
To provide a model-based prediction of individual urinary glucose excretion (UGE) effect of ipragliflozin, we constructed a pharmacokinetic/pharmacodynamic (PK/PD) model and a population PK model using pooled data of clinical studies.
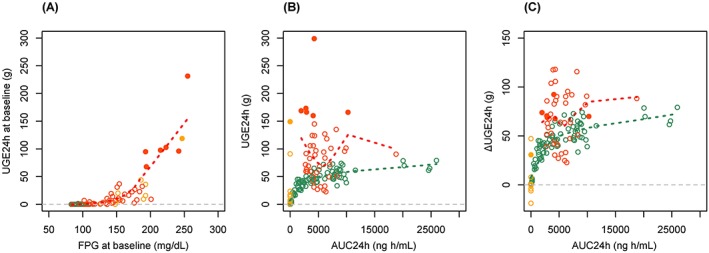
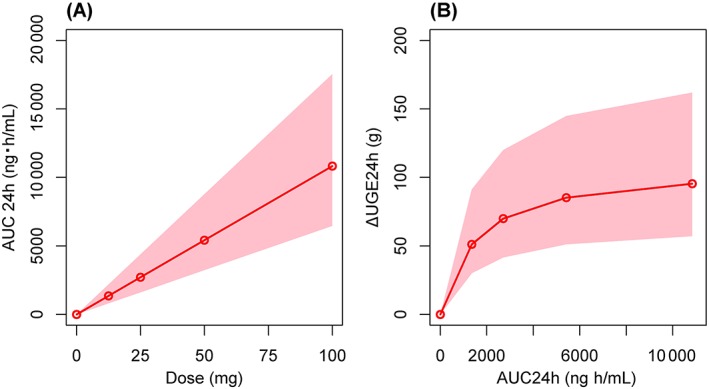
A PK/PD model for the change from baseline in UGE for 24 hours (ΔUGE ) with area under the concentration-time curve from time of dosing to 24 h after administration (AUC ) of ipragliflozin was described by a maximum effect model. A population PK model was also constructed using rich PK sampling data obtained from 2 clinical pharmacology studies and sparse data from 4 late-phase studies by the NONMEM $PRIOR subroutine. Finally, we simulated how the PK/PD of ipragliflozin changes in response to dose regime as well as patients' renal function using the developed model.
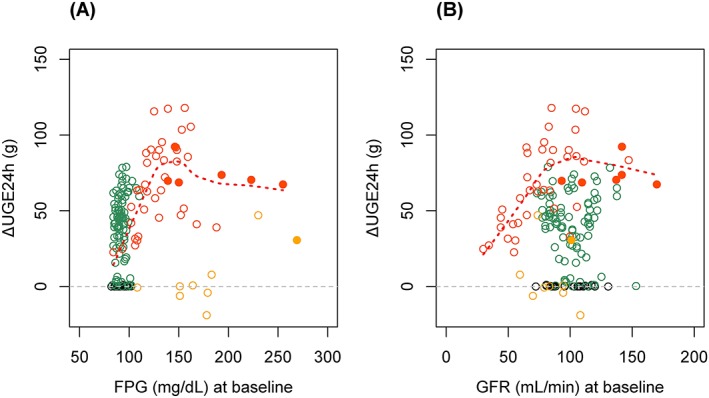
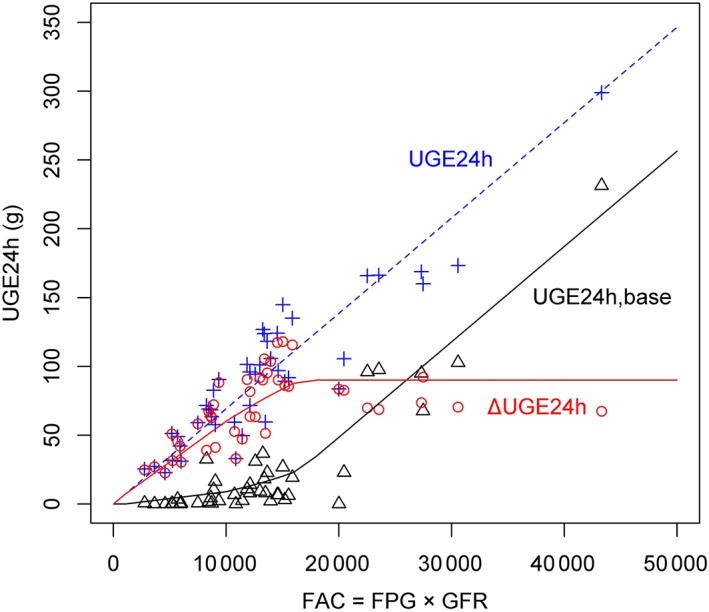
The estimated individual maximum effect were dependent on fasting plasma glucose and renal function, except in patients who had significant UGE before treatment. The PK of ipragliflozin in type 2 diabetes mellitus (T2DM) patients was accurately described by a 2-compartment model with first order absorption. The population mean oral clearance was 9.47 L/h and was increased in patients with higher glomerular filtration rates and body surface area. Simulation suggested that medians (95% prediction intervals) of AUC and ΔUGE were 5417 (3229-8775) ng·h/mL and 85 (51-145) g, respectively. The simulation also suggested a 1.17-fold increase in AUC of ipragliflozin and a 0.76-fold in ΔUGE in T2DM patients with moderate renal impairment compared to those with normal renal function.
The developed models described the clinical data well, and the simulation suggested mechanism-based weaker antidiabetic effect in T2DM patients with renal impairment.
通过对来自临床研究的汇总数据进行药代动力学/药效学(PK/PD)模型和群体 PK 模型构建,为依帕列净的个体尿糖排泄量(UGE)效应提供基于模型的预测。
采用最大效应模型描述依帕列净 24 小时 UGE 从基线变化(ΔUGE)与给药后 24 小时内浓度-时间曲线下面积(AUC)的 PK/PD 模型。使用 2 项临床药代动力学研究中的丰富 PK 采样数据和 4 项后期研究中的稀疏数据,通过 NONMEM $PRIOR 子例程构建群体 PK 模型。最后,我们使用开发的模型模拟依帕列净 PK/PD 如何响应剂量方案以及患者肾功能的变化。
个体最大效应的估计取决于空腹血糖和肾功能,但在治疗前有明显 UGE 的患者除外。2 型糖尿病(T2DM)患者的依帕列净 PK 可通过具有一级吸收的 2 室模型准确描述。群体平均口服清除率为 9.47 L/h,在肾小球滤过率和体表面积较高的患者中增加。模拟表明 AUC 和 ΔUGE 的中位数(95%预测区间)分别为 5417(3229-8775)ng·h/mL 和 85(51-145)g。模拟还表明,与肾功能正常的患者相比,中度肾功能不全的 T2DM 患者的依帕列净 AUC 增加 1.17 倍,ΔUGE 降低 0.76 倍。
所开发的模型很好地描述了临床数据,模拟表明肾功能不全的 T2DM 患者的降糖作用存在基于机制的减弱。